 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 1, January-February, 2009, pp. 4-6 Indian Perspective Epilepsy surgery in India Kurupath Radhakrishnan R. Madhavan Nayar Center for Comprehensive Epilepsy Care, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum, Kerala, India Correspondence Address: Dr. Kurupath Radhakrishnan, Senior Professor and Head, Department of Neurology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum - 695 011, Kerala, India. krk@sctimst.ac.in Date of Acceptance: 24-Feb-2009
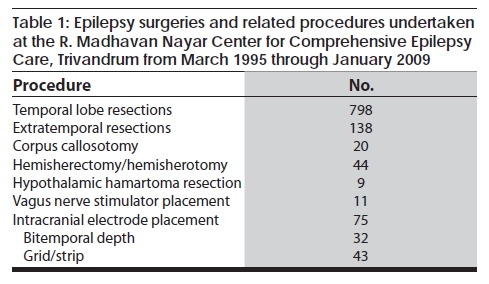
Code Number: ni09003 Abstract This review traces the evolution of epilepsy surgery in India from the beginning to the present state. During the last one and half decades, surgical treatment of epilepsies has made resurgence in this country and at present a few centers have very active and sustained epilepsy surgery programs. Within a 14-year period, the R. Madhavan Nayar Center for Comprehensive Epilepsy Care, Trivandrum, has undertaken over 1000 epilepsy surgeries. However, in the whole country, annually, not more than 200 epilepsy surgeries are currently being performed. This number is a miniscule when compared to the number of potential surgical candidates among the vast population of India. The enormous surgical treatment gap can only be minimized by developing many more epilepsy surgery centers in different parts of our country.Keywords: Developing countries, epilepsy, epilepsy surgery Introduction Nearly one-third of the patients with newly diagnosed epilepsy on long-term follow-up will have their seizures unsatisfactorily controlled by treatment with available antiepileptic drugs. [1] A majority of these patients with difficult to control seizures have focal epilepsies. The remarkable advances in neuroimaging technologies during the past two decades have allowed detection of a variety of brain lesions in over half of the patients with medically refractory focal epilepsies such as hippocampal sclerosis, malformations of cortical development, benign neoplasms, vascular malformations and focal gliotic lesions that are amenable to surgical resections. [2] Epilepsy surgery was considered until recently to be an expensive high-technology therapy restricted to the industrialized world. The understanding that a majority of patients with substrate-directed intracranial lesions associated with chronic focal epilepsies can be selected for surgery based on relatively simple and affordable non-invasive presurgical evaluation strategies has resulted in recent years in the creation of epilepsy surgery programs in developing countries. [3] A recent survey revealed that, in 26 of 142 (18.3%) economically disadvantaged nations, at least one center regularly conducted epilepsy surgeries, compared with 18 of 24 (75%) developed countries. [4] Out of 50 million people with epilepsy globally, 80% live in resource poor countries. [5] India with over one billion people will have over one million people with medically refractory epilepsies, of which nearly one half are potential surgical candidates. The success of an epilepsy surgery depends upon the early identification of potential surgical candidates, and selecting from them, ideal candidates destined to have a postoperative seizure-free outcome. Since epilepsy surgery centers in developing countries will lack the full range of state-of-the-art technologies usually available in the developed world to perform presurgical evaluation and surgery, the success of epilepsy surgery programs in a developing country set-up will depend upon the ability to select ideal surgical candidates using locally available technology and expertise without compromising on patient safety. [6],[7] Despite major challenges, in the last one and half decades, a handful of epilepsy surgery centers in India have not only successfully implemented epilepsy surgery programs, but have also produced results comparable to those from developed countries at a fractional cost. On January 14, 2009, the R. Madhavan Nayar Center for Comprehensive Epilepsy Care (RMNC) at Trivandrum, Kerala, performed the 1000 th epilepsy surgery. Through this brief review, I intend to trace the evolution of epilepsy surgery in India and discuss its present state. Ancient India Archeological excavation of trephined skulls from the pit-dwellers of Burzahom in the northwestern Himalayan region (present day Kashmir Valley) suggests that trephination might have been practiced in prehistoric India (4000 to 4300 years ago) for acquired neurological ailments. One particular skull of a female from Burzahom, first discovered in 1968, revealed 11 attempts at trephination, with 6 neatly completed circular or oval perforations, all in the left parietal bone. [8] The left calvarium showed hypertrophy, which could have been related to long-standing atrophy of the underlying brain. It was impossible to establish the precise symptoms that may have afflicted this individual, but the Burzahom female might have been ′insane, epileptic or otherwise different′. [8] The carefully performed trephination, suggestive of a multistage procedure on a possibly anomalous skull, argues for a surgical approach for medical reasons on a living person. It is also likely that this might have been part of a ritual in a primitive society that regarded epilepsy and other neurological diseases to be a result of demonic possessions. About 2000 years ago in India, medical practice was based on Ayurveda , and shalya chikitsa (surgical treatment) was one of its major branches. [9] The sage Sushruta was a master surgeon of his times, and his surgical techniques have been documented in the Sushruta Samhita . Although well versed in many aspects of surgery, no specific references to epilepsy surgery have been made in Sushruta Samhita . The Modern Era of Epilepsy Surgery in India The beginning and initial enthusiasm The first epilepsy surgery in India was performed on August 25, 1952, by Dr. Jacob Chandy at the Christian Medical College (CMC), in Vellore, on a 19-year old male, hailing from Trichur, central Kerala, who had right infantile hemiplegia and medially refractory seizures (personal communication, Professor V. Rajshekhar, Head of Department of Neurosurgery, CMC, Vellore). The patient died on the ninth day after a left hemispherectomy due to meningitis. During the 1950s, 1960s, and the first half of the 1970s, several patients with uncontrolled epilepsies were operated on at CMC, Vellore, [10],[11],[12] and at the Institute of Neurology, Madras. [13],[14] The localization of the epileptogenic focus was based on seizure semiology as obtained from history records, data from a scalp interictal EEG, and radiological investigations available then such as a skull radiograph, pneumoencephalogram, and carotid angiogram. In a recent retrospective analysis of 141 patients operated for epilepsy at CMC, Vellore, 102 (73%) had temoral resections, 23 (16%) had extratemporal resections, and 16 (11%) had multilobar resections. [15] At the Institute of Neurology, Madras, steriotactic lesions were made in the amygdalo-hippocampal region for temporal lobe epilepsy and in the centro-median nucleus of the thalamus, the field of Forel, and in the internal capsule for generalized seizures and infantile spasms. [13],[14] The Decline In the mid-seventies, like elsewhere in the world, epilepsy surgery took a dramatic downward trend in India as well. The retirement from active service of Dr. Jacob Chandy and Dr. Ramamurthi from the centers they almost single handedly developed, less than expected postoperative seizure outcome, availability of more effective antiepileptic drugs, and stigma associated with epilepsy surgery due to its mistaken identity with psychosurgery collectively contributed to this decline. The Resurgence The author returned to India in 1994 after having been trained at the Epilepsy Program, Mayo Clinic, Rochester, Minnesota, USA and started the RMNC at the Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum, Kerala. The first epilepsy surgery (left anterior temporal lobectomy with amygdalohippocampectomy) at RMNC was conducted on March 20, 1995. The patient was a 25-year old male with left mesial temporal sclerosis and medically refractory complex partial seizures. The break up of epilepsy surgeries performed in RMNC is provided in [Table - 1] . Almost simultaneously, epilepsy surgery programs were started at the All India Institute of Medical Sciences, New Delhi, and the National Institute of Mental Health and Neurosciences, Bangalore. During the last one and half decades, these three centers together have undertaken over 1500 epilepsy surgeries which is several fold more than the epilepsy surgeries performed in India during the previous four and half decades. There are half a dozen other centers in the country doing less than 20 epilepsy surgeries per year. The published outcome data from major epilepsy surgery centers in our country are comparable to those from developed countries. [16],[17],[18],[19],[20],[21] In evolving the most productive surgery program in India today, the RMNC has given due emphasis to the following special issues relevant to surgical treatment of epilepsies in resource poor countries. First, epilepsy surgery cannot be performed occasionally on an isolated basis, but must be an uninterrupted well-defined program that utilizes a systematic approach with established criteria for patient selection, surgery and follow-up. Second, the decision making for epilepsy surgery needs a multidisciplinary approach in which different investigators involved with the program such as a neurologist with extensive experience in clinical epileptology and EEG, a neurosurgeon with expertise in epilepsy surgery, a neuroradiologist with special interest in epilepsy imaging, a dedicated video-EEG monitoring technologist, a psychologist, a psychiatrist and a medical social worker work in conjunction to create an integrated picture of epileptogenesis and its impact on the patient and care givers. Knowing when not to operate because of the need for further investigations is an important as selecting which patient may benefit from surgery with limited facilities available. Epilepsy surgery centers in developing countries should initially restrict their surgical candidates to patients with mesial temporal lobe epilepsy and those with circumscribed potentially epileptogenic lesions in whom the epileptogenic zone can be unquestionably localized by using locally available relatively inexpensive and noninvasive technologies, and in whom excellent postoperative outcome can be guaranteed. Third, it is important for epilepsy surgery centers to regularly assess their capabilities and limitations and adopt a stepwise approach to increasing levels of complex presurgical evaluation and surgical treatment strategies. Forth, after temporal lobe resective epilepsy surgery, there is over 70% probability that the patient will be seizure-free and over 30% chance of being free of antiepileptic drugs within two years after surgery. [17] A seizure-free person could be better employed and become a productive member of the society. Indian Epilepsy Society and epilepsy surgery centers in our country could effectively use these statistics to attract governmental and non-governmental financial supports for providing subsidized surgery to the underprivileged. Last, if the surgery program is to have a lasting impact, it would be essential to work with and educate the local professionals and public about the recent advances in the treatment of epilepsies. In India with over 500,000 potential epilepsy surgery candidates, not more than 200 epilepsy surgeries per year are being undertaken today. Thus only a miniscule of potential surgical candidates in our country ever gets a chance to undergo presurgical evaluation and surgery. This enormous surgical treatment gap can only be minimized by developing many more epilepsy surgery centers in India. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09003t1.jpg] |
| |||||||||


{kind=link}