 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 1, January-February, 2009, pp. 58-60 Case Report Prosopagnosia: A rare presenting manifestation of frontotemporal lobar degeneration Arun George, James Jose Department of Neurology, Medical College, Calicut, Kerala - 673 008, India Correspondence Address: Dr. Arun George, Department of Neurology, Medical College, Calicut, Kerala - 673 008, India. a.george@rediffmail.com Date of Acceptance: 06-Feb-2009
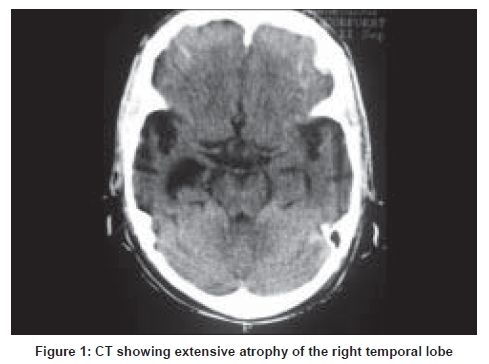
Code Number: ni09014 Abstract Frontotemporal dementia is an important neurodegenerative disorder accounting for a significant proportion of dementia cases with onset before 60 years of age. Apart from the well recognized behavioral changes the disease has many other distinctive features like predominant language involvement alone or associated features of motor neuron disease or parkinsonism etc. which at times may be the presenting manifestation itself. In the following article we describe a rare presenting manifestation; prosopagnosia, in the setting of frontotemporal degenerationKeywords: Frontotemporal degeneration, prosopagnosia Introduction Frontotemporal dementia (FTD) is an important neurodegenerative disorder accounting for approximately 50% of dementia cases presenting before 60 years of age. The term FTD was introduced by workers in Lundh (Sweden) and Manchester (UK) to refer specifically to the progressive behavioral syndrome. Later researchers found that the syndrome of FTD was not confined to behavioral changes alone, but can also affect the language domains. Subsequently, in 1998, the Neary criteria were put forward which recognized three clinical syndromes: 1) FTD 2) Progressive nonfluent aphasia 3) Progressive fluent aphasia (semantic dementia). In addition to the three clinical syndromes recognized by Neary and colleagues there is increasing recognition of other clinical features that can occur in the setting of frontotemporal lobar degeneration (FTLD). These include aphasic syndromes that do not meet the Neary criteria, parkinsonism, motor neuron disease (MND), corticobasal degeneration, progressive supranuclear palsy, and prosopagnosia. We describe a rare presenting manifestation in the setting of FTLD. Case Report A 55-year-old male presented with an 18-month history of progressive difficulty in recognizing familiar faces. Initially he could identify them by their voices, but later he could not identify them by their voices or even after the individual's name had been mentioned to him. He had a difficulty in identifying some common objects encountered in day to day life. His behavior and language was normal and he had no impairment of executive function, memory, praxis, and visuospatial problems. He did not have any weakness, Parkinsonism, bulbar symptoms or alien limb phenomenon. There was no family history of any significant illness and there was no history of any trauma or psychiatric illness. Examination showed a right-handed, conscious, cooperative and attentive person. Formal neuropsychological tests, namely Mini Mental Status Examination (MMSE) and a standard neuropsychological battery devised to explore memory, language, praxis, and executive functions, visual and space perception was normal except rare circumlocution in the language domain. The most marked abnormality was his difficulty in recognizing familiar faces. He could not match names to faces and he failed to give any details concerning the named persons including his close friends and relatives. He also had some difficulty in identifying common objects and could not identify blue color. His routine blood, urine examinations, blood sugar, renal and liver function tests and a chest X-ray were normal. A computed tomographic scan showed marked atrophy of the nondominant frontotemporal lobe [Figure - 1]. Electroencephalogram was normal. A lumbar puncture showed normal cerebrospinal fliud pressure, < 5 cells (all mononuclear cells), protein 65mg/dl and sugar 45mg/dl. He was seen last at 21 months into his illness when he still had the cross-modal agnosia subtle behavioral changes of excessive anger, irritability and rare wandering episodes. Discussion This patient presented with prosopagnosia. The term prosopagnosia was coined by Bodamer in 1947. It refers to the inability to recognize familiar faces. The lesions that cause prosopagnosia are usually found in the ventral occipitotemporal cortex involving the fusiform and lingual gyrus [1] and are bilateral in most cases although right unilateral lesions [2] can cause the syndrome. The criteria for the prosopagnositic variant of FTD defined by Neary et al ., [3] include I. Core diagnostic features A. Insidious onset and gradual progression B. Perceptual disorder characterized by
II. Supportive diagnostic features A. Pressure of speech B. Idiosyncratic word usage C. Surface dyslexia and dysgraphia III. Brain imaging (structural and/or functional): Asymmetric abnormality predominantly affecting nondominant (right) anterior temporal lobe. Our patient satisfies the core criteria and the imaging features. But our patient has a cross-modality loss of person recognition than simple prosopagnosia in that he cannot recognize persons by their voices or even after their name has been mentioned. A survey of the literature showed that at least in some of the cases reported as progressive prosopagnosia the recognition disorder is not confined to face recognition but rather represents a cross-model impairment of person knowledge i.e. semantic knowledge. [4],[5] In this context the understanding of how the human brain perceives and recognizes faces becomes important. Studies have shown that faces activate the bilateral fusiform gyrus although the most robust activity is seen on the right side. This region has been referred to as a fusiform face area (FFA) and is defined as a module of face perception. [6] Similarly, voices have been found to activate the bilateral superior temporal gyrus, more on the right. [7] These two modalities may access the semantic store independently or they may converge to form a multimodal association area for person recognition from which they may access the semantic store. In our patient the initial inability to recognize faces with preserved recognition by voices and names suggests damage to the right FFA. Subsequent inability to recognize persons by voices suggests damage to the auditory processing area. The final stage where he is unable to recognize a person by any modality suggests damage to the semantic store itself. The list of clinical features associated with atrophy of frontal and temporal lobes is increasing. What is the link between the varying clinical features and the common denominator i.e. frontotemporal atrophy is not clear. Future research may shed light upon this and thus open up new therapeutic targets for this disabling illness. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09014f1.jpg] |
| |||||||||

{kind=link}