 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 1, January-February, 2009, pp. 63-65 Case Report Reversible cerebral vasoconstriction syndrome Monica Saini, T. Jeerakathil, K. Butcher Department of Neurology, University of Alberta, Canada Correspondence Address: Dr. T. Jeerakathil, Department of Neurology, University of Alberta, Canada, T6G2B7. thomasj@ualberta.ca Date of Acceptance: 30-Jan-2009
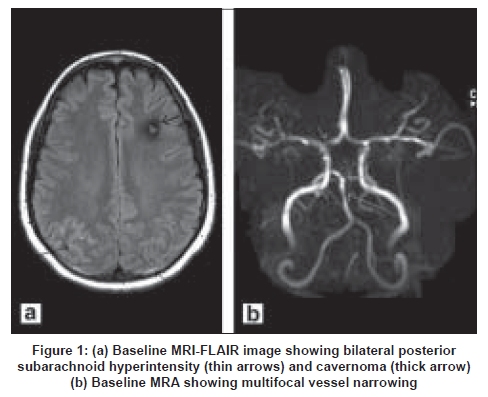
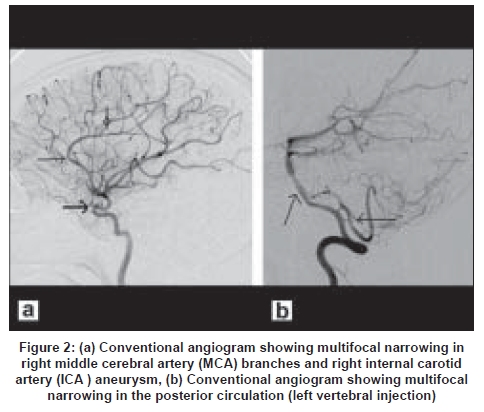
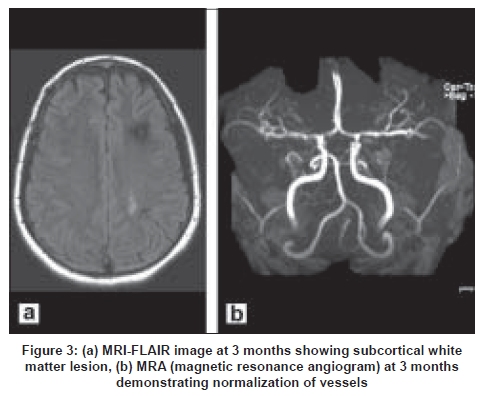
Code Number: ni09016 Abstract Reversible cerebral vasoconstriction syndromes (RCVS) are a group of disorders that have in common an acute presentation with headache, reversible vasoconstriction of cerebral arteries, with or without neurological signs and symptoms. In contrast to primary central nervous system vasculitis, they have a relatively benign course. We describe here a patient who was diagnosed with RCVS.Keywords: Reversible, vasculitis, vasoconstriction Introduction Reversible cerebral vasoconstriction syndrome (RCVS) is a recently proposed term which unifies a variety of previously described syndromes including benign angiopathy of the central nervous system (CNS), migrainous angiitis, drug-induced angiopathy, post-partum angiopathy and the Call-Fleming syndrome. [1] We report here the clinical course and radiological findings in a patient who was diagnosed with RCVS. Case Report A 37-year-old woman presented with complaint of a single episode of severe headache. Headache was explosive in onset and recovered over few hours. In the preceding two weeks, there had been intermittent episodes of dizziness. Past medical history was significant for migraine without an aura, smoking, ovarian carcinoma and bilateral salpingo-oophorectomy. She was taking low-dose oral hormonal (estrogen) replacement since her surgery 15 years ago. There was no history of illicit drug use or preceding use of sympathomimetics, triptans or antidepressants. On physical exam, pulse rate was normal; blood pressure was 150/80mm Hg. The cardiovascular, respiratory and abdominal examination was unremarkable. Neurological exam did not reveal any abnormalities. Computerized tomography (CT) scan of the brain performed one day after the onset of headache showed an incidental left frontal cavernoma, without evidence of acute bleed. Magnetic resonance imaging (MRI) performed on the same day revealed FLAIR (fluid attenuated inversion recovery) hyperintensities overlying bilateral posterior parietal-occipital regions [Figure - 1]. In view of the possibility of cortical subarachnoid hemorrhage (cSAH), four-vessel angiogram DSA (digital subtraction angiography) was performed to rule out underlying arteriovenous abnormalities. The DSA revealed two paraclinoid aneurysms (2-3mm) in the left internal carotid artery (LICA). Multifocal constriction involving bilateral large and small vessels was noted in bilateral anterior and posterior circulations [Figure - 2]. The vasoconstriction was presumed to be secondary to a recent aneurysmal bleed, and coil embolization of the aneurysms was attempted, which was unsuccessful. Operative exploration did not reveal intradural aneurysms in the LICA; moreover, the arachnoid in the area did not show blood staining. Postoperatively, the patient had two episodes of moderate headache, temporally correlated to straining, which resolved over 1-2h. In view of operative findings, aneurysmal bleed was thought to be unlikely and vasoconstriction was attributed to an angiopathy. Laboratory investigations showed ESR of 11, normal C-reactive protein and complement levels, and were negative for syphilis (rapid plasma regain), antinuclear antibody and rheumatoid factor. Lumbar tap performed postoperatively revealed normal glucose, 10 white blood cells (WBCs, 80% polymorphs) and protein 1.57g/dl. No clinical or laboratory evidence for an underlying vasculitic process was forthcoming. A possible diagnosis of RCVS was considered. The patient received intravenous methylprednisolone (three doses, 1g/day), followed by tapering doses of oral steroids over the next four weeks. Post-discharge, she reported few episodes of transient dizziness, without focal neurological deficits, over a period of one month. A follow-up MRI of the brain, performed three months after the index event, showed a single lesion (hyperintense on T2 and FLAIR) in the left parietal sub-cortical area [Figure - 3a]. MR angiography showed normalization of vessel abnormalities [Figure - 3b]. Discussion Reversible cerebral vasoconstriction was described by Call and colleagues in a series of patients presenting with acute headaches with or without neurological deficits; previously there had been isolated case reports. [2] It has been reported in benign angiopathy of the CNS, migraine, thunderclap headache, in post-partum women and in relation to use of vasoactive medications and recreational drugs. [1],[3],[4] These have often been confused with primary CNS vasculitis because of similar clinico-radiological features that include headache, focal neurological deficits (transient episodes or stroke) and abnormalities evident on cerebral angiography. RCVS has been recently used as a unifying term for these syndromes, though there is still a lack of a clear definition or diagnostic criteria. [1] The pathophysiology of RCVS is not yet clearly understood. An abnormality in the regulation of cerebral vascular tone is thought to be responsible. This may be primary, or secondary to exogenous factors including drugs, trauma and endocrine abnormalities. [1] Though female predominance and relation to post-partum state seem to indicate a role of sex-hormones in the pathogenesis of RCVS, the relation is not clear. Typically, patients with RCVS are young (20- 50 years), predominantly female (female : male 1.8 : 1). [1],[4] The commonest clinical presentation is severe acute headache, often thunderclap headache, with or without focal deficits or seizures. Headache as the sole presenting symptom is reported in approximately 76% of cases. Headache may be associated with nausea, vomiting and photosensitivity. Precipitating factors are identifiable in almost 60% cases and include post-partum state, uncontrolled hypertension and the use of nasal decongestants, anti-depressants, cocaine, cannabis, interferon and nicotine patches. Other neurological symptoms include transient visual or sensory symptoms, aphasia, hemiparesis, ataxia, seizures and stroke. Headaches tend to recur over a period of days-weeks. Our patient presented with a thunderclap headache, with recurrences over a period of one week. Cerebrospinal fluid (CSF) analysis is normal in most; 10-50% show abnormalities including protein elevation (generally < 0.8mg/l) and mild increase in white cell count (< 10/mm 3 ). Brain imaging is normal in a majority of patients; in others, cSAH or parenchymal hemorrhages may be seen at baseline. [4],[5] Ischemic stroke tends to occur in/following the second week. [4] In a few patients, reversible posterior-predominant lesions in the white matter may be identified, possibly secondary to vasogenic edema. Neurovascular imaging in patients with RCVS shows diffuse, segmental vasoconstriction involving large and medium-sized vessels. Beading in multiple vascular beds, with areas of dilatation, is characteristic. The most specific finding is the resolution of angiographic abnormalities within days- weeks (12 weeks). In our patient, though CSF was mildly abnormal, it was thought to be secondary to craniotomy; another possibility was protein exudation secondary to distal angiopathy. The location of FLAIR hyperintensities was atypical for an aneurysmal bleed, and was similar to imaging findings previously described in RCVS. The diffuse vasoconstriction, involving both anterior and posterior circulation, reversed within 12 weeks. The treatment of RCVS is guided by observational data. Good outcomes have been reported with the use of short-course steroids, calcium channel blockers and magnesium sulfate. Some patients have done well with observation alone. [1],[4] Clinically, RCVS has a benign course. Stroke, ischemic or hemorrhagic, may be seen in 7-54% of patients. Cortical subarachnoid hemorrhages (cSAH) have been reported in 22% of patients in a single case series, and are more common in females. [4] In general, hemorrhagic complications tend to occur early in the course, and are thought to reflect a distal, small-vessel angiopathy. Our patient received short-term steroids and had an excellent outcome. The single FLAIR lesion, seen on the follow-up MRI, was clinically asymptomatic. It is important to distinguish RCVS from CNS vasculitis, which has an aggressive course and mandates long- term use of immunosuppression. Most patients with RCVS have a background of good health and present with hyperacute/acute severe headache, unlike primary CNS vasculitis where patients present with progressive headache with/without cognitive dysfunction. The definitive distinguishing feature of RCVS is the reversibility of vasospasm within days-weeks. In patients with CNS vasculitis, though mild improvement may occur, reversibility of vascular abnormalities is not seen. The difficulty lies in differentiation of the two in the early phase, especially in terms of decisions regarding therapy. In patients presenting with thunderclap headache, normal CSF results and typical angiographic abnormalities, observation or use of calcium channel blockers is justified. However, in patients without the typical presentation, use of short-term steroids to cover both possibilities, seems prudent. In conclusion, our patient presented with features typical of RCVS, and the diagnosis was confirmed by demonstrating reversibility of vasoconstriction. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09016f3.jpg] [ni09016f2.jpg] [ni09016f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}