 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 1, January-February, 2009, pp. 66-68 Case Report Balò's concentric sclerosis presenting with benign clinical course and multiple sclerosis-like lesions on magnetic resonance images Yongmei Li, Peng Xie1, Xiao Fan, Huamin Tang Departments of Radiology and 1Neurology, the First Affiliated Hospital, Chongqing Medical University, Chongqing, China Correspondence Address: Dr. Peng Xie, Departments of Radiology and Neurology, The First Affiliated Hospital, Chongqing Medical University, Chongqing, China. xiepeng58@21cn.com Date of Acceptance: 21-Jan-2009
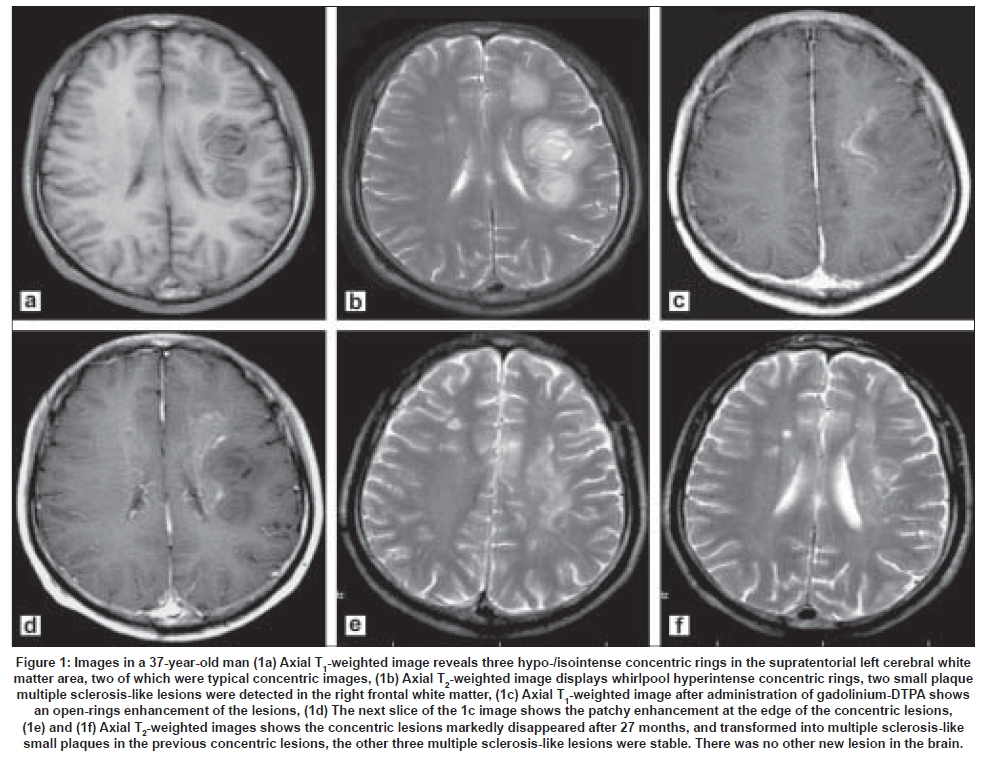
Code Number: ni09017 Abstract Balò's concentric sclerosis (BCS) is a rare primary demyelinating disease of central nervous system (CNS) and is considered to be a variant of multiple sclerosis (MS). It is characterized by a severe, rapidly evolving course with CNS lesions consisting of concentric rings of demyelination alternating with myelination in the white matter. We report a patient with BCS from mainland China diagnosed on magnetic resonance imaging (MRI) findings. In addition to two contrast enhanced open ring lesions. MRI also showed multiple small white matter lesions in both the hemispheres. The patient had a good response to corticosteroids and had a benign prognosis during a follow-up period of two years.Keywords: Concentric sclerosis, magnetic resonance imaging, multiple sclerosis Introduction Balò first described the histological features, alternating bands of loss and partially preserved myelin, of this clinical enitity, Balo's concentric scleriosis (BCS). Earlier reports suggested lethal outcomes, but magnetic resonance imaging (MRI) has changed this view and long-term survival has been reported with BCS. [1] More recent reports suggest a benign evolution with spontaneous remission. [1],[2],[3],[4],[5] Of the less than 80 cases reported in the literature, most involved young male adults. More cases are from the Asian countries, China, India, and Turkey suggesting possible role of genetic and environmental factors. [2],[3],[4],[5],[6],[7] We report a patient with BCS from mainland China with MRI follow-up. Case Report A 37-year-old male was admitted with dizziness and numbness and weakness of right side limbs. Neurological examination revealed loss of orientation to time and place, poor calculation ability and memory disturbance. He also had right supranuclear facial paralysis, right hemiparesis and hemisensory loss. Cerebrospinal fluid (CSF) examination was abnormal: cell count 27/mm 3 and protein 54mg/dL. CSF immunoglobulin G index was normal and there was no oligoclonal bands. Visual and brainstem auditory evoked potential studies were normal. Brain MRI, T 2 -weighted and fluid-attenuated inversion recovery (FLAIR) images showed three lamellar concentric mass lesions are in the white matter of left hemisphere, one in the frontal lobe and two in the periventricular area. On contrast-enhanced MRI, two of the lesions had open-ring enhancement. The maximal diameter of the lesions was 4.0 cm. Interestingly, three small multiple sclerosis-like lesions were also seen, two in the right periventricular white matter and the other in the left lateral ventricular triangle-area [Figure 1 a-d]. Patient received 1000mg/day intravenous methylprednisolone for five consecutive days. He had improvement in his clinical symptoms at one month follow-up. There was no relapse in the symptoms during the next 27 months of follow-up. Follow-up at 27 months showed mild memory disturbances and a follow-up MRI showed resolution of the ring lesions and small plaques in the previous regions [Figure 1 e, f], and the three multiple sclerosis-like lesions were stable. No new lesions were seen. Discussion BCS is a rare primary inflammatory demyelinating disease of the central nervous system. Pathologically, it is characterized by a peculiar pattern of alternating rings of myelin preservation or remyelination and myelin loss, consistent with demyelination, involving the cerebral hemispheres, cerebellum, brainstem and spinal cord. Diagnosis can also be established by biopsy. [6] Stadelmann et al ., investigated the immunopathology of BCS. [8] Active concentric lesions followed a pattern of demyelination which resembled hypoxia-tissue injury. Recent MRI studies also support this hypothesis. [9] The diagnosis of BCS is based on clinical signs and symptoms, exclusion of other neurological diseases and the characteristic concentric rings lesions seen by MR images. BCS has characteristic MRI features; hypo-/isointense concentric rings on T 1 -weighted image; multiple whirlpool hyperintense concentric rings on T 2 -weighted image, and open-ring enhancement of the lesions with Gadolinium. Our patient in addition had small multiple sclerosis-like demyelinating plaques. Advanced neuroimaging can provide important in vivo markers of disease progression. [9] Proton spectroscopy may show high choline peak and low a decrease peak of N-acetylaspartate peak, similar to acute MS plaques. BCS is considered a rare and acute variant of MS. Our case confirms the earlier observation that BCS can have a benign course without relapses [2],[3],[4] Shankar et al . reported a clinically silent case of BCS in a patient with an oligodendroglioma. [7] The important differential diagnosis of BCS includes acute disseminated encephalomyelitis. A similar configuration of MRI lesions can be seen occasionally during an exacerbation of MS. However, the typical concentric pattern on MR images as described above is highly suggestive of BCS. High dose of steroids may not change the rapidly progressive clinical course of BCS, but most patients have been treated successfully with immunosuppressive drugs. Plasma-exchange and immunosuppressive therapy followed by autologous stem cell transplantation can also be utilized. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09017f1.jpg] |
| |||||||||


{kind=link}