 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 1, January-February, 2009, pp. 76-78 Case Report Olfactory ensheathing cell tumor Kaushal Ippili, Boola G. Ratnam, Swarnalata Gowrishankar1, Alok Ranjan, Rahul Lath Departments of Neurosurgery and 1Pathology, Apollo Hospitals, Jubilee Hills, Hyderabad - 500 033, Andhra Pradesh, India Correspondence Address: Dr. Rahul Lath, Department of Neurosurgery, Apollo Hospitals, Jubilee Hills, Hyderabad - 500 033, Andhra Pradesh, India rahullath@hotmail.com Date of Acceptance: 05-Feb-2009
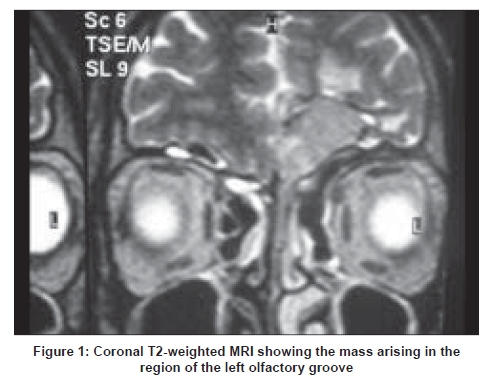
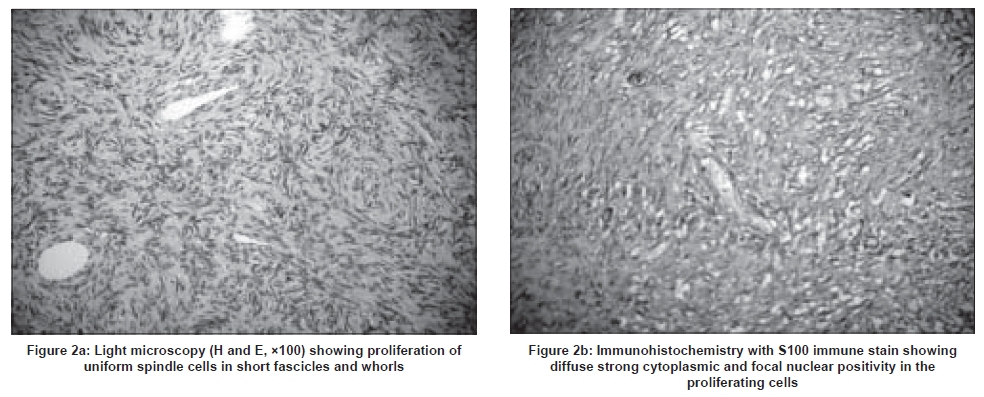
Code Number: ni09020 Abstract Olfactory ensheathing cells (OECs) are found in the olfactory bulb and olfactory nasal mucosa. They resemble Schwann cells on light and electron microscopy, however, immunohistochemical staining can distinguish between the two. There are less than 30 cases of olfactory groove schwannomas reported in the literature while there is only one reported case of OEC tumor. We report an OEC tumor in a 42-year-old male and discuss the pathology and origin of this rare tumor.Keywords: Brain tumor, olfactory ensheathing cell tumor, olfactory schwannoma Introduction Olfactory ensheathing cells (OECs) have the characteristics of both astrocytes and schwann cells. [1] They ensheathe olfactory axons and have the unique ability to regenerate and have been successfully applied in different experimental models aimed to repair damaged cord. [2] OECs are similar to Schwann cells in light and electron microscopic appearance, however, immunohistochemical staining can distinguish between the two. [3] Olfactory groove schwannomas are extremely rare, only 30 cases have been documented in the English literature, we could find only one reported case of OEC tumor. [3] We report a case of olfactory groove tumor showing features consistent with an OEC tumor. Case Report A 42-year-old man presented with history of multiple episodes of generalized tonic clonic seizures. There were no neurocutaneous markers. Olfaction was normal and there were no focal neurological deficits. Computerized tomography (CT) scan of the brain showed an extra-axial isodense mass in the left subfrontal region which enhanced homogenously with contrast. On magnetic resonance imaging (MRI) the lesion was isointense on T1-weighted images and mildly hyperintense on T2-weighted images and fluid-attenuated inversion recovery sequence [Figure - 1]. He underwent a left frontal craniotomy and excision of the tumor. It was a partly suckable and fibrous tumor arising from the left olfactory bulb. Light microscopy showed spindle cells arranged in short fascicles, palisades and whorls. The cells were spindled out with curved vesicular nuclei and ill-defined cytoplasmic margins [Figure - 2a]. On immunohistochemical staining the cells were strongly positive for S100 protein [Figure - 2b] and negative for epithelial membrane antigen (EMA), glial fibrillary acidic protein (GFAP) and smooth muscle actin (SMA). However the tumor cells were negative for CD57 (Leu7). The immunohistochemical studies suggested that the cell of origin of the tumor was OEC rather than the Schwann cell. Patient is doing well at one-year follow-up and postoperative CT scan showed complete excision of the lesion. Discussion OECs share features of both Schwann cells of the peripheral nervous system (PNS) and astrocytes of the central nervous system (CNS). During development OECs emerge from the olfactory placode while Schwann cells from the neural crest, thus sharing a common peripheral origin. [1] Both cell types are known to express a number of different molecular markers in common, display a similar morphological phenotype in culture and respond to the same growth-promoting molecules. [1] Recent studies show that OECs have been successfully isolated from the human olfactory bulb and olfactory mucosa. [4] Studies have shown that OECs express smooth muscle protein alpha actin both in vitro and in vivo which provides evidence that these cells are quite different from Schwann cells. [5] These cells are similar to Schwann cells on light and electron microscopy. [3] On immunohistochemical staining Schwann cells are positive for S100 and Leu7 (CD57) while OECs are positive for S-100 and negative for Leu7 (CD57). [3] Both are negative for EMA differentiating them from meningiomas. Olfactory groove and subfrontal schwannomas are rare tumors with lesser than 30 cases reported in the literature, of which six have been from India. [6],[7],[8],[9],[10],[11] The CNS does not possess Schwann cells and therefore the origin of this tumor has been debated. These tumors may arise from the olfactory bulb and nerve or an intracranial peripheral nerve closely associated with the olfactory nerve. [12] Occasionally, an intracranial schwannoma may arise at a site not related to a cranial nerve. The origin of these tumors could be from 1) hyperplasia of the Schwann cells localized within the perivascular nerve plexuses, 2) meningeal branch of the trigeminal nerve in the anterior cranial fossa, 3) anterior ethmoidal nerve around the cribriform plate, 4) hamartomatous lesion consisting of Schwann cells as a result of displaced neural crest cells and 5) reactive changes after injury whereby Schwann cells arise from multipotent mesenchymal cells after injury. [13] Schwannomas at this location are preoperatively misdiagnosed as meningiomas, ethesio-neuroblastomas and dural-based metastases. [11],[14] The presence of bone scalloping and the absence of bone sclerosis and a dural tail may help in differentiating it from a meningioma. [14] A case of cystic olfactory groove schwannomas has also been reported. [8] A recent report has suggested that T2-weighted MRI sequence may help in distinguishing meningioma from schwannoma. [11] Presence of multiple foci of low signal intensities (related to microbleeds) in T2-weighted MRI may point towards a schwannoma. Yasuda et al. , reported a patient with OEC tumor. [3] They used immunohistochemistry to differentiate it from a schwannoma. These authors have suggested that OECs are the origin of subfrontal /olfactory groove tumors rather than the Schwann cell as seen in our patient. Using this hypothesis, some of the previously reported olfactory groove schwannomas may have been OEC tumors. The use of tumor markers (S100 and CD57) as an adjunct to microscopy would help in differentiating these tumors. Surgical excision remains the mainstay of treatment and total excision is considered curative. Radiation therapy has been used for residual schwannomas at this location. [9] References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09020f2.jpg] [ni09020f1.jpg] |
| |||||||||


{kind=link}
{kind=link}