 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 1, January-February, 2009, pp. 79-81 Case Report Persistent primitive hypoglossal artery associated with lower basilar artery aneurysm: Diagnosis and clinical implications Sunil V. Furtado, Kalyan Reddy1, Nilesh Khandelwal1, A. S. Hegde Departments of Neurosurgery and 1Radiology, Sri Satya Sai Institute of Higher Medical Sciences, Bangalore, India Correspondence Address: Dr. Sunil V. Furtado, Department of Neurosurgery, Sri Satya Sai Institute of Higher Medical Sciences, EPIP Area, Whitefield, Bangalore - 560 066, India. sunilvf@gmail.com Date of Acceptance: 20-Jan-2009
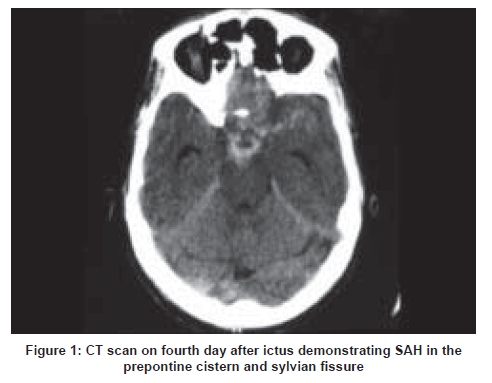
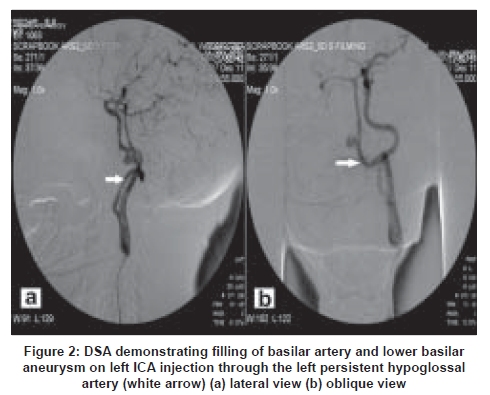
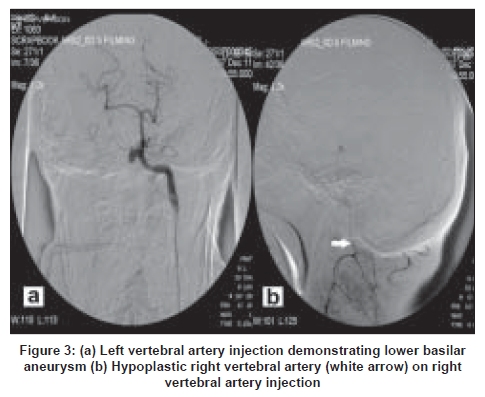
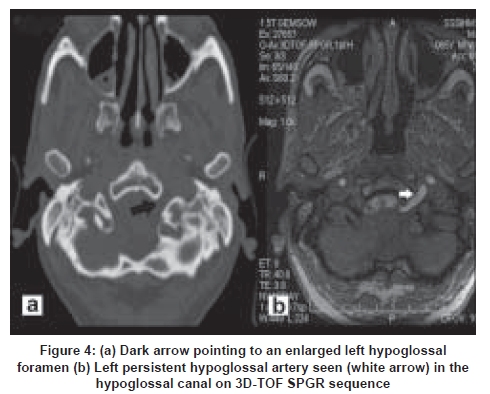
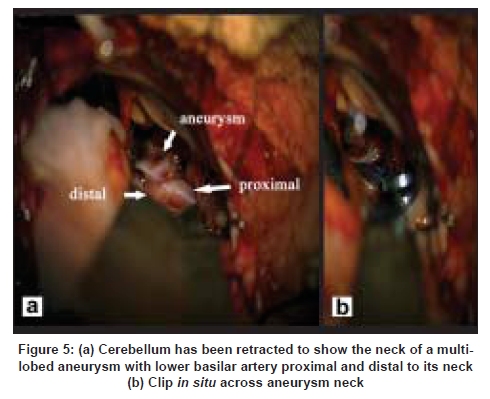
Code Number: ni09021 Abstract An elderly male was evaluated for subarachnoid hemorrhage and found to have a persistent primitive hypoglossal artery with its associated abnormal posterior fossa circulation and a lower basilar artery aneurysm. Angiography findings are described and are corroborated with computed tomography and magnetic resonance imaging. Its surgical and clinical relevance are discussed.Keywords: Basilar artery, hypoglossal, intracranial aneurysm, subarachnoid hemorrhage Introduction During embryogenesis, anastomoses are formed between the carotid artery and the basilar or the vertebral artery, which regress with maturity of the vertebral artery. A persistent primitive hypoglossal artery (PHA), which is a segmental vessel, is a rare anomaly. It usually represents an incidental finding in cerebral angiograms and is associated with unique anomalies of posterior fossa circulation. This embryonic remnant is clinically significant when associated with aneurysm or atherosclerotic disease of the posterior circulation. [1] About 30 cases of posterior circulation aneurysms associated with PHA are documented in English literature. Case Report A 65-year-old male with no significant past medical history presented with severe headache, vomiting and loss of consciousness. A plain computed tomogram (CT) scan done at the referring hospital on the fourth day of ictus revealed Fisher Grade II bleed with blood in the prepontine, ambient cisterns and sylvian fissures [Figure - 1]. There was no intraventricular blood or hydrocephalus. He was started on nimodepine (60mg 4 hourly), dexamethasone 4mg 8 hourly, promethazine 25mg 8 hourly, phenytoin 100mg 8 hourly and kept well hydrated. Two weeks after referral to our hospital he had improved and was in Hunt and Hess Grade I, with no significant neurological signs. A digital substraction angiogram (DSA) revealed a PHA on the left side, arising from the cervical internal carotid artery (ICA) at C2-3 level [Figure - 2 a,b]. It was seen on left ICA injection and entered the posterior fossa at the region of the hypoglossal canal and joining the basilar artery (BA) at the lower clivus [Figure - 2 a,b]. The right vertebral artery (VA) appeared hypoplastic [Figure - 3b]. Both posterior communicating arteries (PCOM) were not visualized on right, left ICA and VA injections. There was a narrow-necked multi- lobulated saccular aneurysm in the lower BA segment, 9 x 5 x 11mm in size, projecting horizontally to the right and filling on left ICA and left VA injection. Rest of the intracranial circulation was normal. The left hypoglossal canal was wider compared to the right [Figure - 4a]. Magnetic resonance (MR) 3D-TOF SPGR sequence showed a large vessel entering the posterior fossa through the left hypoglossal canal [Figure 4b]. MR imaging (MRI) and MR angiography (MRA) were done to qualify the anatomical relationship between the abnormal posterior circulation, aneurysm, brainstem and bony posterior fossa structures. The patient underwent a right lateral suboccipital craniectomy. Anesthesia was maintained with a combination of isofluorane, propofol, fentanyl and vecuronium. He was administered 1.5g methyl-prednisolone at craniotomy and 0.5g/kg body weight of mannitol at durotomy for cerebral protection. Cerebellar retraction exposed petrous dura and lower cranial nerves. The aneurysm was adherent to dura on lower clivus and was approached between the lower cranial nerves. The aneurysm was distal to the formation of the BA, from the union of the PHA and left VA and above the left posterior inferior cerebellar artery (PICA). There was no evidence of vasospasm. The aneurysm was dissected off the dura and clipped uneventfully, after visualizing the BA, proximal and distal to the aneurysm [Figure - 5 a,b]. Mean blood pressure was maintained around 60-65 mm Hg during dissection and clipping. Aneurysm fundus was not excised. Apprehensions existed regarding the visualization of BA and aneurysmal neck in the clival midline due to subarachnoid inflammation. However, drainage of cisterna magna cerebrospinal fluid and a reverse Trendelenberg position allowed retraction of a lax cerebellum and proper visualization. Patient had an uneventful postoperative period and did not have any lower cranial nerve deficits or intrinsic brainstem signs. He was kept on triple-H regimen for a week after surgery along with Nimodepine. Discussion PHA, with an incidence of 0.03-0.26% of cerebral angiograms is the second most common carotid basilar anastomosis, after persistent trigeminal artery. [1] Its presence can be explained by the carotid basilar anastomosis which develops between the anterior and posterior circulation in the 4-5mm embryo, as the vertebral arteries are not yet formed. [2] The segmental anastomotic channels like the trigeminal, otic and hypoglossal are named after the nerve they accompany. Failure of involution of segmental anastomosis beyond the 40th day, when the PCOM are well developed, leads to their sporadic presence. [1] The anomaly, first described in 1889, is most often demonstrated during angiography for sub-arachnoid hemorrhage (SAH), arteriovenous malformations, ischemic cerebrovascular events and tumors. [2],[3] Lie [4] laid down four criteria for identification of PHA: a) it arises from the cervical part of the ICA at the C1-C2 level; b) it enters the posterior cranial fossa via the hypoglossal canal, c) basilar trunk must fill distal to the anomalous vessel and d) absent PCOM. [4] However, recognition of the artery in noninvasive imaging is important. The artery widens the hypoglossal canal on CT and tomograms. [5] The vessel can also be demonstrated entering through the hypoglossal canal and joining the BA using CT or MR angiography. These are acceptable diagnostic alternatives especially in incidentally detected cases. [6] 3D-CT angiography and MRA may not detect multiple small unruptured aneurysms and aneurysms such as PCOM segment aneurysms. [6] DSA remains the gold standard in the event of SAH, to localize the aneurysm and qualify the flow through abnormal posterior circulation and circle of Willis. PHA has been variously associated with aneurysms of the BA, PICA and also PHA. The anomalous structure of the vessel wall of PHA exposes the basilar trunk to unusual hemodynamic stress and development of aneurysms. [1],[7] Kempe and Smith described a syndrome presenting with pain in the tonsillar fossa and posterior part of the tongue due to close association of the lower cranial nerves with PHA. [8] Because of its origin from the ICA and associated flow dynamics at the carotid bulb, atherosclerotic plaques can be expected. [9] A typical distribution of emboli can lead to clinical dilemma. [1] Associated hypoplasia of vertebral arteries and PCOM predisposes to a precarious posterior fossa circulation, making it susceptible to various surgical and thromboembolic insults. For all functional purposes, PHA may be the only dominant posterior fossa arterial supply. [7] Careful understanding of the abnormal vasculature is important during aneurysm or skull-base surgery, carotid endarterectomy or endovascular intervention. Proper delineation of parent vessel proximal and distal to the aneurysm is important before clipping of aneurysms. In our case, this was necessitated because of a poor communicating supply across PCOM. Surgery is a formidable challenge in view of perilous circulation and site of aneurysm. Temporary clips proximal and distal to the aneurysm may be placed on the PHA, VA and BA respectively for a short period, with cerebral protection in the event of a rupture. Ligation of the PHA in such cases can have disastrous consequences. Aneurysm arising from PHA has been coiled using access through the residual segmental anomaly. [10] Stent-assisted coiling is also a mode of treatment of these aneurysms. This modality provides a better chance of having a patent posterior circulation without concomitant surgical morbidity. Surgery can be considered in the event of complications or failure of endovascular treatment. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09021f3.jpg] [ni09021f1.jpg] [ni09021f5.jpg] [ni09021f2.jpg] [ni09021f4.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}