 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 1, January-February, 2009, pp. 88-90 Case Report Spinal epidural cavernous hemangioma with myelopathy: A rare lesion D. K. Satpathy, S. Das, B. S. Das Departments of Neurosurgery and Pathology, Kalinga Hospital, Bhubaneswar, Orissa, India Correspondence Address: Dr. D. K. Satpathy, Kalinga Hospital, Chandrasekharpur, Bhubaneswar, India drdksatpathy@rediffmail.com Date of Acceptance: 13-Feb-2009
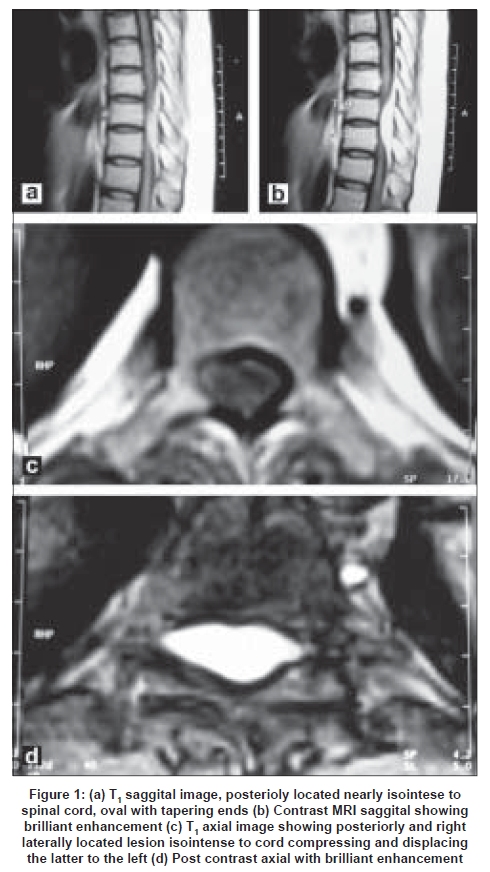
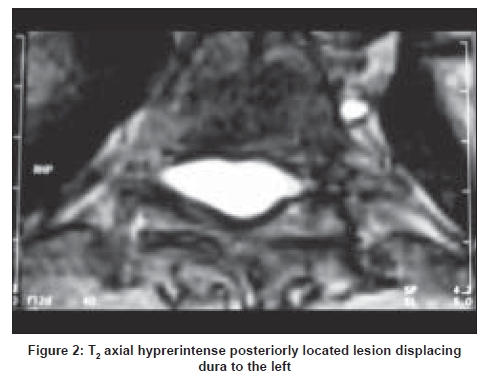
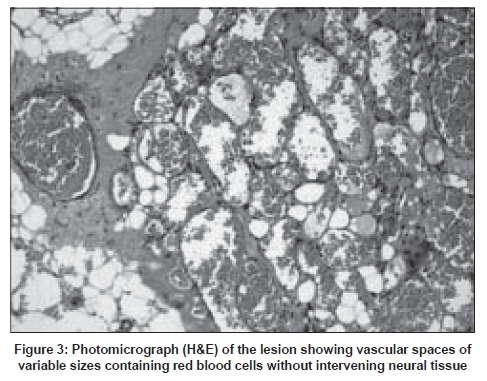
Code Number: ni09024 Abstract A case of pure epidural cavernous angioma involving the dorsal region of the spine is presented. The clinical picture was of a slowly progressive compressive myelopathy. Imaging studies only showed a dorsally located epidural mass lesion. Histology confirmed the diagnosis of this rare type of lesion. The patient improved after excision of the lesion.Keywords: Spinal, epidural, cavernous hemangioma Introduction Cavernous angioma, also known as cavernous malformation, cavernous angioma or cavernoma is a developmental vascular anomaly. It forms about 8-15% of all developmental cerebro-vascular malformations. Spinal cavernous angiomas are rare lesions and particularly so the epidural ones. Our case is one of such type without osseous involvement in the dorsal region of the spine. From a review of the literature only 80 cases of spinal epidural cavernous angiomas without primary origin in the vertebrae could be evaluated. [1],[2] Case Report A 42-year-old gentleman presented with progressive spastic weakness of both lower limbs, right followed by the left leg, since six months. Two months prior to admission he could walk only with one stick support. He had no urinary disturbances and no pain. General examination revealed no abnormality. Patient was alert and upper limbs had no neurological deficit. Right lower limb power was Grade 3/5 and that of left was Grade 4/5. The lower limbs were spastic with hypoesthesia below T 10 segmental level on both sides. There was no spinal tenderness or deformity. Sphincters were normal and other systemic examination revealed no abnormality. All routine blood investigations were within normal limits. Plain radiographs of dorsal spine did not show any bony abnormality. Magnetic resonance imaging (MRI) of dorsal spine revealed an extradural compressive lesion at T 9-10 level on right side displacing the dura to the left. It was isointense on T 1 , iso to hyperintense on T 2 and brilliantly enhancing with contrast [Figure - 1],[Figure - 2]. Keeping with this profile a differential diagnosis of a meningioma was considered; however, other rare possibility of extramedullary hemopoetic conditions was also considered. The patient underwent laminectomy from T 8 to T 10 . There was an epidural pinkish mass dorsally located extending to the right side and displacing the dura to the left. It had a longitudinal extent of about 5 cm; with a good cleavage from the dura. The mass was slowly lifted off. No dural attachment was noted. The tumor in the lateral side of the spinal canal could be removed with ease. There was neither extra-spinal extension nor any bony involvement. Macroscopic total excision was achieved. The excised lesion was brownish red soft tissue measuring 2 x 1 x 0.5cm; cut section showed spongy appearance. Microscopic examination revealed a tumor composed of vascular spaces of variable sizes with fibro-collagenous wall lined by a single layer of flattened epithelial cells. The lumina contained red cells and the intervening area in between the vascular spaces did not reveal any neural or parent tissue. Fibro-fatty connective tissue was seen in between lobules of vascular spaces. The histological feature was characteristic of cavernous angioma [Figure - 3]. The patient progressively improved and could walk a few steps unaided at the time of discharge. Subsequently, he recovered completely. During follow-up for six years, the patient has been doing well and leading a normal life. Repeat MRI one year after surgery revealed no residual or recurrence of the lesion. Discussion Cavernous angiomas or cavernomas comprise a group of developmental vascular malformations. It can occur anywhere in the central nervous system. They form about 7% of all vascular malformations, and spinal vascular malformations form 3-12% of spinal space-occupying lesions. [3],[4] It can be solitary or multiple and may be associated with similar lesions in other organs of the body. In a large series of MR scans, multiple lesions were detected in 18.7% of cases. [5] The location of the lesion was vertebrae, extradural, dural, subpial and intramedullary. [4] The cavernous angiomas occur throughout the brain, spinal cord and meninges. About 80% of the cavernous angiomas are supratentorial, 15% infratentorial and 5% are located in the spine. [3] The cavernous angiomas occur in two forms: sporadic and familial. Ten per cent of all cavernomas are familial forms, most of the rest are sporadic. [6] Pure epidural cavernous angiomas are extremely rare. Only 80 cases could be evaluated from the literature till 2006. [1],[2] In the spinal region the cavernous angiomas may be confined to the vertebrae, vertebral lesions secondarily extending into the spinal canal, purely epidural or purely intramedullary in location. Lesions at all sites reveal identical features on light and electron microscopy as well as in immunohistochemistry. [7] Cavernous angiomas are composed of sinusoidal vessels, adjacent to one another without intervening mother tissue. These are well-circumscribed lesions with discrete borders, dark to purple in color, and can be multilobulated. There may be calcification and thrombosis. The blood flow in these lesions is slow and therefore, not visualized in standard angiography. [3] Hemorrhages are common in intra-axial lesions but less frequent in extra-axial ones. [8] The usual clinical presentation is that of a slowly progressive spinal cord compression. Rarely, there may be acute compressive features due to associated extradural hemorrhage. [9] Our patient had short duration of para-paresis and clinically thoracic myelopathy was suggested. MRI is the investigation of choice. Computed tomography scan may show a hyperdense or calcified lesion on plain study. There may be minimal or no enhancement with contrast. MRI shows T 1 isointense and T 2 iso to hyperintense signal changes. Contrast enhancement frequently occurs. [10] Bleeding inside the tumor is rare though occurs, when there may be T 1 hyperintense signal within it. The usual differential diagnoses are that of meningioma, hemopoetic disorders or metastasis. Microsurgical excision of symptomatic lesions in accessible locations is the treatment of choice. [9] This is possible for most of the lesions located posteriorly. When total excision is not possible adjuvant radiotherapy is advised. [11] Our patient recovered completely after total excision of the extradural lesion. From the available MRI scans, including the repeat scan one year after surgery, there has been no evidence of a second lesion or recurrence. At surgery an all-out attempt was made to remove the lesion completely. No adjuvant therapy was given. The case is reported because of its rarity and difficulty in making a preoperative diagnosis without a coexisting bone lesion. Acknowledgment The authors thank Dr. Asima Prusty for her editorial assistance. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09024f2.jpg] [ni09024f1.jpg] [ni09024f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}