 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 1, January-February, 2009, pp. 100-101 Neuroimage Giant hemispheric multiloculated brain abscess Wen-ke Liu, Lu Ma, Bo-yong Mao Department of Neurosurgery, West China Hospital, Sichuan University, Chengdu, Sichuan Province, P.R. China Correspondence Address: Dr. Boyong Mao, Department of Neurosurgery, West China Hospital, Sichuan University, Chengdu, Sichuan province, 610 041, P.R. China liuwenke781103@yahoo.com.cn Date of Acceptance: 26-Jan-2009
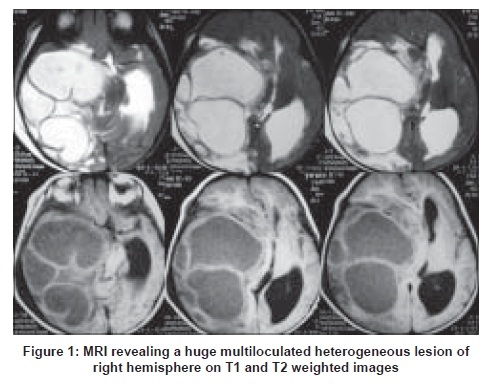
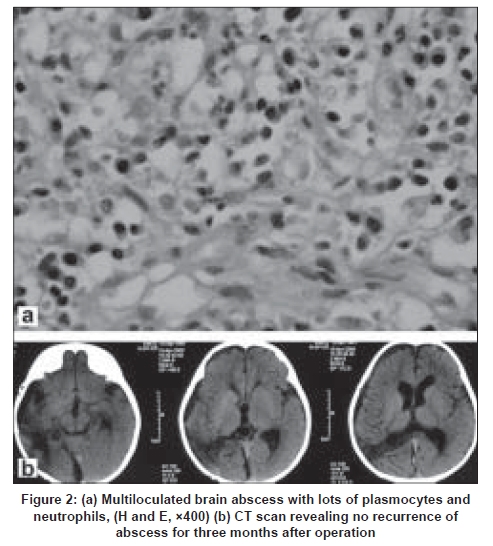
Code Number: ni09033 A two-year-old baby was reffered to pediatric clinic for decreased appetite, pharyngeal congestion and lethargy. The pediatrician made a diagnosis of pharyngitis. Vital signs were normal and neurological examination revealed decreased muscle tone in the left sided limbs and right ptosis. The left pupil diameter was 2mm whereas it was 5mm on the right side. The white blood cell count was 8.04 x 10 9 /L with differential counts of 67% neutrophils. Magnetic resonance imaging (MRI) revealed a giant cerebral hemispheric multiloculated lesion, which was hypointense on T1-weighted image and hyperintense on T2 [Figure - 1]. The preoperative diagnosis was cystic glioma or other ill-defined diseases. During the operation, a thick-walled giant multiloculated abscess containing thick pus was seen. The pus grew Staphylococcus aureus . Pathological examination also confirmed brain abscess [Figure - 2a]. Patient recovered well without any neurological defect post-operatively. Follow-up computed tomography (CT) scan done at three months revealed no residual abscess [Figure - 2b]. Differentiation between multiloculated brain abscess and cystic brain tumors such as low-grade glioma is often difficult with conventional and diffusion MRI. [1] In our patient the brain abscess was possibly of otogenic origin as the child had pharyngeal inection, in the past which could easily lead to tympanitis and hemispheric brain abscess. This is because the short and wide auditory tube in a child can get easily infected. Surgical treatment should be attempted for reducing the mass effect, obtaining the pathologic diagnosis, and identifying infecting pathogens for facilitating selection of antibiotics. [2] Excision seemed to be the most appropriate surgical choice for multiloculated abscess as recommended by Loftus et al . [3] References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09033f1.jpg] [ni09033f2.jpg] |
| |||||||||

{kind=link}
{kind=link}