 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 1, January-February, 2009, pp. 102-103 Neuroimage Cavernous sinus thrombophlebitis causing reversible narrowing of internal carotid artery K. S. Madhusudhan, Harsh Kandpal, Jitesh Ahuja Department of Radiodiagnosis, All India Institute of Medical Sciences, New Delhi - 110 029, India Correspondence Address: Dr. Harsh Kandpal, Senior Research Associate, All India Institute of Medical Sciences, New Delhi - 110 029, India. drharshk@yahoo.com Date of Acceptance: 26-Jan-2009
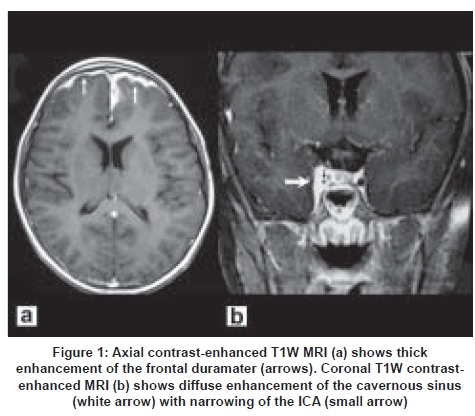
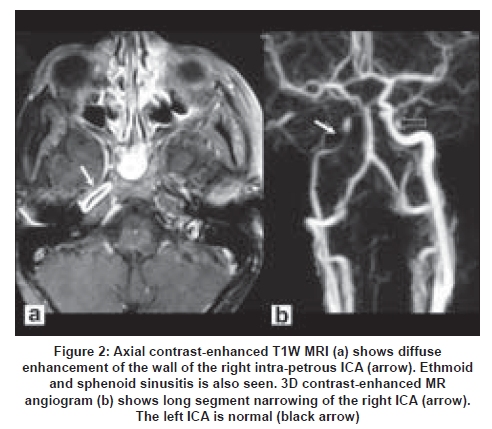
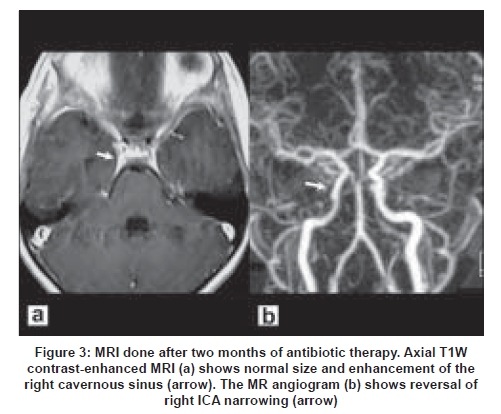
Code Number: ni09034 A nine-year-old boy presented with eight-days history of progressive frontal headache, high-grade fever, periorbital swelling and proptosis. Clinical examination showed tenderness in the region of frontal sinus, chemosis and restricted right ocular movements. Contrast-enhanced magnetic resonance imaging (MRI) performed with the clinical suspicion of cavernous sinus thrombophlebitis (CST) showed mucosal enhancement of all the paranasal sinuses and frontal pachymeningitis [Figure 1a]. The right cavernous sinus was enlarged and also showed contrast enhancement [Figure 1b]. The wall of the petrous segment of the right internal carotid artery (ICA) showed diffuse enhancement [Figure 2a]. 3D contrast-enhanced MR angiogram (MRA) revealed diffuse smooth narrowing of the cavernous and petrous segments of internal carotid artery (ICA) [Figure 2b]. Based on the imaging features, a diagnosis of pansinusitis causing right CST, arteritis and narrowing of intra-cavernous ICA, and frontal pachymeningitis was made. The patient was started on broad-spectrum antibiotics. Follow-up MRI performed two months later showed resolution of sinusitis, CST and restoration of ICA caliber to normal [Figure 3]. Cavernous sinus thrombophlebitis is a rare, potentially lethal condition which still has a mortality of about 30%. [1] The cavernous sinus has extensive valveless communications with many facial and neck veins which can serve as conduits for spread of infection. Infection typically spreads from the adjacent paranasal sinuses, particularly sphenoid and ethmoid sinuses, face, orbit or teeth. Staphylococcus aureus is the most common causative organism. [1] Infection of the cavernous sinus may present as fever, ptosis, proptosis, chemosis, cranial nerve palsies, headache and periorbital edema. [1] Neurological sequelae may occur uncommonly in the form of ophthalmoplegia, blindness, hemiparesis and pituitary insufficiency. [2] Involvement of the ICA is uncommon and occurs in the form of stenosis, occlusion and aneurysm formation. [2],[3] Although the location of the ICA within the cavernous sinus may indicate that its involvement is likely in cases of CST, in practice, it is seldom seen. The inflammation involves the arterial wall, leading to stenosis, luminal thrombosis and aneurysm formation due to the weakening of the wall. Stenosis may also develop secondary to compression of the artery by the adjacent thrombosis. [1] The major role of imaging is in detection of the cause and extent of inflammation. Computed tomography (CT) scan and more importantly, MRI has contributed significantly towards diagnosis. [1] Direct signs of CST include enlargement of the sinus with a lateral bulge, and multiple irregular filling defects. [4],[5] Indirect signs include enlargement of the tributary veins, particularly superior ophthalmic vein, exophthalmos, soft tissue edema and abnormal dural enhancement of the lateral wall of the sinus. [5] In addition, the source of infection in the paranasal sinuses, orbit or mastoid can be demonstrated. MR angiography is essential for the evaluation of ICA. The mainstay of treatment in CST is systemic administration of broad-spectrum antibiotics. [1] Therapy has to be continued for about three to four weeks after the signs of infection have ceased. Surgery is needed for the management of primary cause or complications. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09034f1.jpg] [ni09034f2.jpg] [ni09034f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}