 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 2, March-April, 2009, pp. 151-156 Original Article Anterior subaxial cervical spine fixation using a plate with single screw per vertebral body: A simple and efficient construct - Clinical series and a cadaver study Prasad S. S. V. Vannemreddy1,2 , Alan Ogden2 , Debi Mukherjee2 1 Departments of Neurosurgery, NIMS-Hyderabad, India Correspondence Address: Dr. Prasad Vannemreddy, Department of Neurosurgery, LSUHSC, 1501 Kings’ Highway, Shreveport, LA 71103. prasad4458@hotmail.com Date of Acceptance: 31-Mar-2009
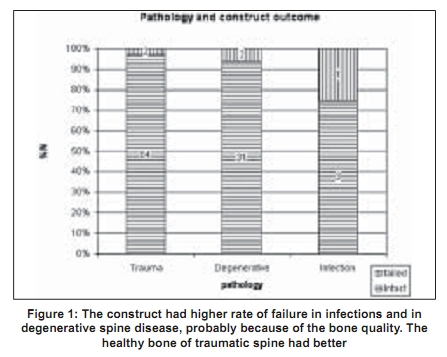
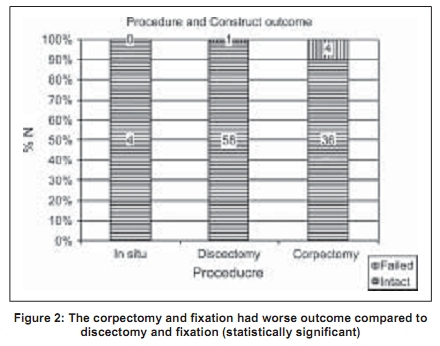
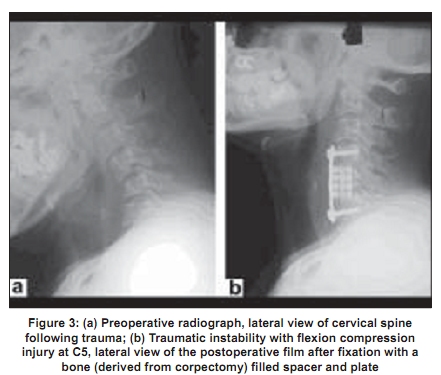
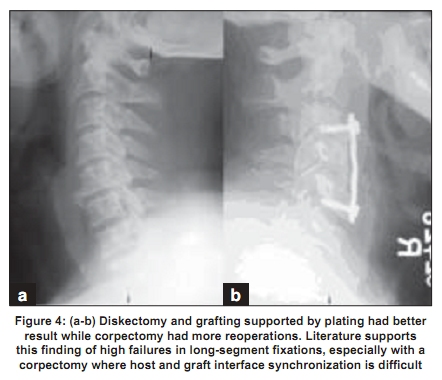
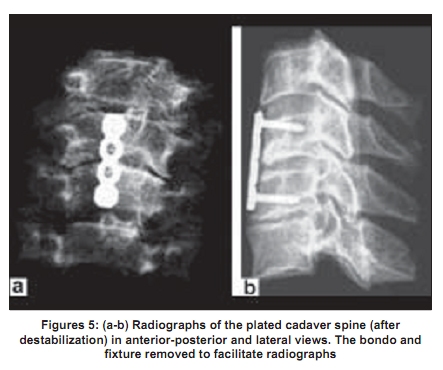
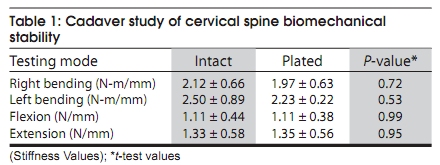
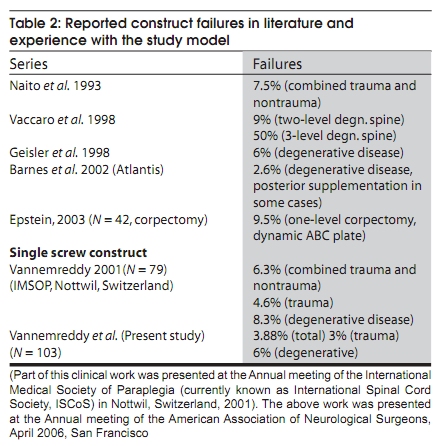
Code Number: ni09044 PMID: 19439844 DOI: 10.4103/0028-3886.51283 Abstract Objective: To report our experience with a novel construct for traumatic and nontraumatic cervical spine lesions that was validated by biomechanical studies of cadaver cervical spine. Study Design: Consecutive cases of anterior cervical spine fixation performed over six years reviewed for stability offered by a construct comprising of a plate fixed by a single screw to each vertebral body.Setting: A university hospital and a biomechanical lab. Materials and Methods: Data were coded and entered into a statistical worksheet for multivariate analysis. Cadaver spine models applied for biomechanical study of stability. Results: Total of 103 cases reviewed; 86 with single-level disease; traumatic in 66 (64%) cases and degenerative in 33 (32%) cases, including hard disks, OPLL, and spondylitis (4% with other causes). Fixation was with diskectomy in 59 and with corpectomy in 40. A bone graft was utilized for fusion in 87 and a bone-filled titanium spacer in 13. A single screw was placed in each vertebral body with a locking plate (having linear arrangement of holes). This construct remained strong in 95% of cases at the end of 6-24 months. Five cases failed requiring reoperation. Five patients with cervical spinal cord injury (SCI) died. On statistical analysis, construct was stronger with diskectomy compared with corpectomy. Construct used on cadavers confirmed the biomechanical stability in short segment fixation (C5-6). Conclusion: A conservative construct utilizing a single screw per vertebral body and a one-holed plate system appears to be strong enough to afford stability in both traumatic and nontraumatic lesions of subaxial cervical spine, comparable to others. Keywords: Anterior fixation, cervical spine, construct, subaxial spine Introduction Anterior cervical approach to disk disease of cervical spine was developed by Robinson and Smith and later described by Cloward who also developed several instruments to facilitate the procedure. [1],[2] Over past half century the procedure had undergone technical refinements and indications also have increased from the original disk disease to traumatic instability and long segment degenerative diseases. To improve the graft (bone or metal) interface with the vertebral bodies and promote healing by rigid immobilization, anterior cervical plating device has gained widespread favor. Earlier constructs promoted highly rigid plate fixations with a postulation that these plates act as load-bearing devices to promote ideal fusion of interbody grafts with minimal or no graft settling. [3] In multilevel fusions, studies have demonstrated that rigid plate fixation dramatically increases fusion rates. [4],[5],[6] However, for single levels, plating may actually decrease fusion rates and result in inferior clinical outcomes by increasing stress shielding and hold the graft in excess distraction and preventing appropriate graft settling. [7],[8],[9] Even for single-level fusions with and without instrumentation, some authors have reported higher union rates with plating, [6],[10] while others performed without plating. [7] The studies in themselves are not free from drawbacks in terms of uniformity in patient population, instrumentation, and graft techniques, thus making it difficult to propose an universal system for any given disease. It is not yet clear from the available literature, if instrumentation is required at all or if there is a need for a heavily rigid construct, which might also predispose patients to adjacent level disease, early. A simpler version of instrumentation that has worked out very well for degenerative as well as traumatic cervical spine lesions in our experience over a decade and when tested in the laboratory had shown stability without serious limitation of mobility. This study was about early success rate of this simple construct. It is also about the failures that required reoperation in the early postoperative period and not about the fusion rates or the long-term follow-up results. Materials and Methods The material has clinical and cadaver spine biomechanical study data. Clinical material and methods A series of consecutive cervical spine anterior fixation surgeries performed and collected prospectively over eight years, between 1996 and 2004, was reviewed retrospectively. In all these patients, implant with the same principle of fixation was utilized, that is, placing a single screw in each vertebral body with a plate in midline, over the anterior surface of vertebra. Anterior cervical diskectomy and/or corpectomy followed standard operative procedures, performed under general anesthesia and with image-intensifier guidance. All patients received external orthotic support for 4-6 weeks postoperatively. None was immobilized by Halo device after internal fixation of the cervical spine. Age, gender, number of levels, type of disease (degenerative, trauma, infection), nature of implant (diskectomy followed by graft or corpectomy followed by graft), and construct outcome (revised and stable on follow up) were analyzed. Statistical analysis Data were coded and entered in to multivariate logistic regression analysis (Sigmastat version 3.0.1a., Systat Software Inc.) for identification of variables that influenced failure of the construct in terms of reoperation (following fallout of the implant). Cadaver cervical spine biomechanical study Five cervical spines (C4-C7) were harvested from unembalmed specimens with an average age of 85 years (range 79-91 years). The soft tissue was removed from each spine after harvest and the specimen was frozen until mechanically tested. Prior to the day of testing, each spine was thawed and cortical bone screws were inserted to fuse C4 to C5 and C6 to C7. This method of transarticular fixation assured no movement between the fused levels and did not obstruct movement between the levels in question, C5 and C6. After fusing, the distal portion, C6 and C7, was placed in a mold and encased in automotive body filler (Bondo, Atlanta, GA). Before the potting material had fully cured, a small anterior portion of the filler was removed to allow placement of the plates. After fusion and potting, the specimens were kept in a refrigerator overnight to allow the body filler to cure. The following day, the specimens were removed from the refrigerator to achieve room temperature. A custom- fabricated fixture was then fastened to the C4 superior facet followed by testing in an Instron 8874 biaxial testing frame (Instron Corp, Norwood, MA). The modes of testing included flexion, extension, and lateral bending in both the right and left directions. Testing in flexion, the distal portion of the specimen was secured in a vice while facing down on the anterior surface. It was then displaced 3 mm at 0.25 Hertz. Extension testing was conducted at the same displacement and rate with the specimen down on posterior aspect. For both left and right lateral bending, the specimens were held in the same fashion and displaced in the respective left or right directions, 1.5 mm at 0.25 Hertz. These modes were conducted in the intact, disrupted, and implanted specimens. Each mode was tested for five cycles After completing the intact testing, the intervertebral joint was deconstructed by dividing anterior longitudinal ligament, annulus, disk contents, and the posterior longitudinal ligament with a surgical blade. The four modes of testing were once again conducted. Fusion of C5 and C6 was achieved with the use of a four-holed titanium plate and screws provided by Synthes (Synthes Corp, Paoli, PA). The plate dimensions were approximately 33mm x 8mm and 2.6mm in thickness and utilized 2.6mm diameter x 16mm screws in the most proximal and distal holes of the plate. Each specimen was returned to the Instron 8874 and underwent the previous four modes of testing. Statistical evaluation was performed using t-test We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research. Results Clinical experience There were 12 females and 91 males with age range between 12 and 73 years (mean of 39.6; SD 12.9). Single-level involvement was seen in 86 (83.5%), two levels in 11 (10.6%), and 3 levels in 6 (5.8%). Traumatic in 66 cases (64%) and degenerative in 33 cases (32%), including hard disks, ossified posterior longitudinal ligament (OPLL), and spondylitic changes. Four cases had destruction by tuberculosis or malignancy (3.8%). Procedure was an in situ fixation in 3.8%, diskectomy and implant in 59 (57.2%), and corpectomy was required in 40 (38.8%). A bone graft was utilized for fusion in 87 cases (84.5%) and a titanium metal spacer filled with bone harvested during corpectomy was placed for fusion in 13 patients (12.6%). A single screw was placed in each vertebral body with a locking plate (having linear arrangement of holes). Bicortical purchase was secured using image intensifier. This construct remained strong in 95% of cases at the end of follow-up ranging between 6 months and 3 years. In five cases (4.9%) there was construct failure requiring reoperation; two cases with degenerative spine disease (6% of degenerative spine) and two with traumatic instability (3% of trauma) [Figure - 1]. Only one out of 59 cases (1.6%) of diskectomy with plate fixation had a failed implant requiring reoperation, whereas, 4 out of 40 cases (10%) of corpectomy required a revision [Figure - 2]. Five patients died in this series, all of them sustained traumatic cervical spinal cord injury (4.8% for the total number of patients and 7.5% for cervical spinal cord injury). On logistic regression analysis (Sigmastat version 3.0.1a., Systat Software Inc.) construct stability was stronger with diskectomy compared to corpectomy ( P < 0.03). In some patients, the construct was removed once bony fusion was observed on follow-up radiographs, upon request. The implant extraction was also much simpler and quick compared to the other routinely used implants. A case each of traumatic instability and degenerative spinal canal stenosis of cervical spine are illustrated with radiographs [Figure - 3] and [Figure - 4], regarding the status of plate fixation in the early postoperative period. As one would expect with less than 5% reoperations in the early postoperative period, the statistical significance ( P value of less than 5) could not be assessed. Results of biomechanics study on cadaver cervical spine Results from the cadaver study showed that the movements of the plated constructs were not statistically different from intact specimens of all four modes of testing at P -values greater than 0.05. The radiographs show the good profile of the plate with a stable construct [Figure - 5a and b]. Inference The plated constructs had the same properties as the intact specimens. The stability of a destabilized specimen is reconstituted using this system [Table - 1]. Discussion Initially reported by Robinson and Smith, in 1955, anterior cervical diskectomy and fusion has revolutionized surgical treatment of cervical spine disease. [1] Advent of technological and biomechanical studies boosted our understanding of the spine mobility and instrumentation methodology. It has been all along, promotion of solid bone healing without graft complication, the main objective of anterior cervical spine surgery. However, addressing the need for rigid, semi-rigid, or dynamic fixation methods has been long pending and till date we do not have standard of care method for optimum fixation of cervical spine disease, except of traumatic instability which requires a rigid construct for reasons well documented in the literature. [3],[4],[5],[6],[7],[11] A bicortical single screw placed in each vertebral body secured by a locking plate in the early 90s had shown encouraging results in many of our patients. The currently, widely available spine instrumentation technology was only evolving during that time. Even with the availability of other fixation systems from Medtronics, Codman, etc., we continued to use the above described (single screw per vertebral body) construct for various reasons. One among them was our experience with these constructs showing low reoperation rate, good bony outcome, less time-consuming procedure, and an implant with less metal occupying less of the prevertebral space. Removal of the implant was also simpler either for reoperation or after the bony fusion. Cost of the implant was also a considerable constraint in some poor patients (each screw would cost more and the plate by the length). Literature review for reported failures of anterior cervical spine construct failures and the proposed construct reported in the present manuscript have shown encouraging findings [Table - 2]. Unfortunately, most of the reports do not demarcate traumatic instability from degenerative disease of cervical spine. The simple construct was equally stronger and successful. The study was about early failure of the constructs requiring reoperation in the postoperative period and not about the fusion rates and long-term follow-up results. The biomechanical study on the cadaver cervical spines had revealed interesting findings that might be very useful for us clinically. In the study group, the plated specimens had movement parameters almost similar to those of intact spines. This means that the proposed construct also preserves motion in and around the stabilized segments and results in less stiffness. Our next study aims at rating the neck stiffness experienced by patients operated by this system in comparison with the other plates fixed by multiple screws. Undoubtedly, anterior cervical spinal fixation and fusion has come of the age and has become a standard procedure for many lesions of the cervical spine. However, long-term clinical follow-up studies have reported substantial incidence of symptomatic degenerative changes at adjacent segments. In a retrospective radiographic study of 106 patients, Baba et al ., reported increased motion at the disk above the fusion segment in approximately 10% of the patients after an average of 8.5 years. [11] Capen et al ., reported degenerative changes above and below an anterior cervical fusion in 36 of 59 patients (64%) after an average of 3.5 years of follow up. [12] Gore and Sepic reviewed the cases of 146 patients of anterior cervical fusion in a five-year follow-up study and found 78% of the patients reported complete relief and 18% partial relief of neck pain, despite radiographic evidence of spondylitic process at adjacent segments. [13] Further follow up of a subgroup of these patients at an average of 21 years showed that 16 of 48 patients (33%) who initially reported relief of their symptoms developed recurrent symptoms at an adjacent level. [14] These studies suggest that, although anterior cervical fusion produces excellent relief of symptoms, one-third of these patients may expect recurrences of their pain from degenerative changes at adjacent levels if followed long enough. Anterior fusion inevitably restricts the total range of motion of the cervical spine. Adopting a displacement control scheme assumes patients customarily force their necks to bend through a presurgical range and would involuntarily result in increased demands on the adjacent segments. Schulte et al. performed kinematic studies in cadaveric human cervical spines; they found that after anterior-plated single-level fusions, flexion at the upper and lower adjacent segments decreased by 13.1 and 18.6% respectively, compared with intact specimens.[15] Similarly, extension decreased by 29.3 and 4.7%, respectively. Patients may compensate the amount of mobility lost to arthrodesis through distant and more mobile joints without overloading segments immediately adjacent to a fusion. The results of another cadaver study revealed that, a single-level anterior-plated fusion causes segmental stiffening of as much as 2.78 times in flexion at the surgical level, its effect on the immediate adjacent segments is significant in axial rotation and lateral bending. [16] Adjacent level disease is over rated. According to Dr. Volker Sonntag, symptomatic adjacent level disk disease is not common and his experience has been under review and pending publication (Personal communication, 2007). Clinically relevant changes may not be a common observation in routine practice following fusion with the rigid constructs at present. However, an implant that matches normal anatomical biomechanics might be an attractive alternative to the currently available metal constructs, especially for single-level degenerative disease after diskectomy. In a recent review of anterior cervical spine surgery for disk disease by Sonntag group, results were found to be equally good for patients who had fusion and fixation compared to those who had no fusion or fixation. [17],[18],[19],[20],[21],[22] Furthermore, comparative, prospective clinical trials also failed to find a clinical benefit with anterior cervical diskectomy and fustion (ACDF). [7],[8] For a single-level disk disease, however, most surgeons in the United States and Canada still prefer to apply fusion and fixation. This has led to development of biodegradable implants, essentially to prevent graft dislodgement, which also had conflicting results. Brkaric et al ., [23] recently reported early failures with the biodegradable plates; three out of six plates failed (one during the procedure and two in the early postoperative period). Almost 100 years after the introduction of surgery for cervical disk disease, we still do not seem to find a consensus or a system that provides an optimal treatment. A best possible solution between a heavy duty metal construct (the currently practiced wide plates with multiple screws) and a fragile one (the biodegradable plates e.g. Mystic, Medtronics) is yet to come out and the simple but effective implant reported in this communication might be useful till that time. We conclude that a conservative construct utilizing a single screw per vertebral body and a simple one-holed plate system appears to be strong enough to afford stability in both traumatic and nontraumatic lesions of subaxial cervical spine, comparable to other currently used constructs. This is time efficient and could be cost effective and had considerably less metal burden on the spine. The biomechanical properties of the construct offer stability while the mobility properties are close to the intact specimen. Our results also suggest that in single-level lesions this construction can be used safely with complete success. The construction had better stability in cases of diskectomy compared with corpectomy cases. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09044t1.jpg] [ni09044f4.jpg] [ni09044t2.jpg] [ni09044f3.jpg] [ni09044f5.jpg] [ni09044f2.jpg] [ni09044f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}