 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 2, March-April, 2009, pp. 157-161 Original Article Surgical treatment options for cerebral alveolar echinococcosis: Experience in six patients Junyi Wang, Bowen Cai, Chao You Department of Neurosurgery, West China Hospital, Sichuan University, China Correspondence Address: Mr. Chao You, No. 37 Guoxue xiang, Chengdu, Sichuang, 610041, P.R.China wangjunyi305@yahoo.cn Date of Acceptance: 04-Apr-2009
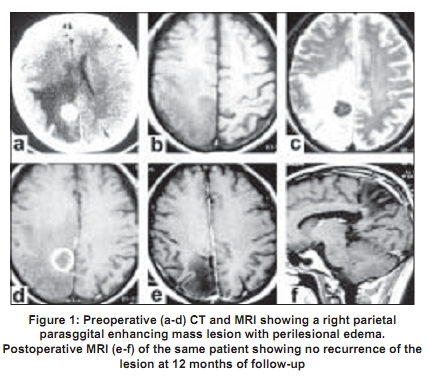
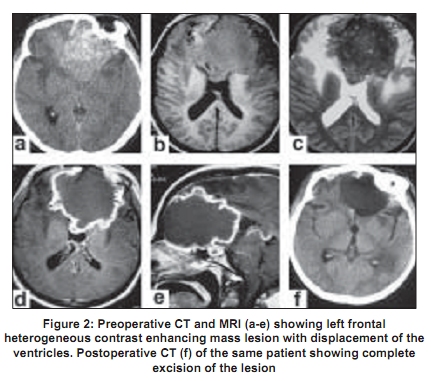
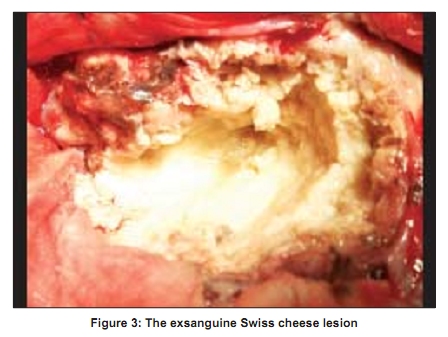
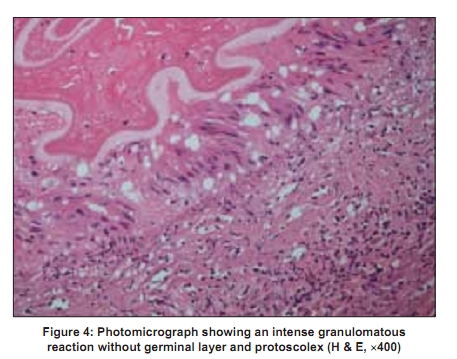
Code Number: ni09045 PMID: 19439845 DOI: 10.4103/0028-3886.51284 Abstract Background: Cerebral alveolar echinococcosis (AE) is a rare but lethal parasitic disease. Its pathogenesis remains poorly understood. Currently there is no widely accepted methods for its surgical treatment.Aims: To discuss the surgical treatment options. Settings and Design: Hospital-based observational study. Materials and Methods: Patients who had surgery for cerebral AE during 2001 and 2007 were the subjects of the study. According to the lesion location and volume, patients have been allocated to either massive resection group or radical piecemeal resection group. Postoperatively, all patients received long-term aldendazole therapy in view of the associated hepatic involvement and were follow-up in the clinic. Results: Of the six patients with cerebral AE who were operated during the study period, four had massive resection and two had radical piece meal resection. None of the patients had postoperative neurological worsening and there was improvement in the neurological status in all the patients except for the patient with blindness. Of the 4 patients in massive resection group, two patients died during the follow-up, one because of liver failure and the other due to hydrocephalus. The remaining four patients were back to their normal activities and none had recurrence of the disease during the follow-up. Conclusions: Although radical massive resection is generally regarded as the surgical method treatment for cerebral AE, radical piecemeal resection can be a reasonable, effective alternative management option, especially when massive resection might result in unavoidable morbidity and mortality. Keywords: Cerebral alveolar echinococcosis, echinococcus multilocularis, surgical treatment Introduction Cerebral alveolar echinococcosis (AE) is a rare life-threatening parasitic disease. Recent investigations have shown increasing prevalence of Echinococcus multilocularis posing a considerable risk in Central Europe, Japan, and China. [1],[2],[3],[4] Currently, radical resection is generally considered as the only method of surgical treatment. [5],[6],[7],[8] However, such an approach at times may be associated with considerable morbidity and mortality. This is much more so when the lesion location is in the brainstem or eloquent areas. We report our experience of surgical treatment for cerebral AE. Materials and Methods Patients operated for cerebral AE between 2001 and 2007 at our hospital were the subjects of the study. All the patients were from north Sichuan, one of the high epidemic regions in China. Definitive diagnosis of cerebral AE was based on the clinical features, operative observations, and pathology. Serological testing for hydotid, Enzyme-Linked ImmunoSorbent Assay (ELISA) was done in all the patients. All patients had computerized tomography (CT) and magnetic resonance imaging (MRI). All patients underwent neurosurgery and were also put on albendazole therapy postoperatively. According to the localization and volume of the lesion, different surgical approaches were performed. Patients were followed-up postoperatively for the outcome of surgery. Results Six patients had surgery for cerebral AE during the study period. The median age was 39 years (range 20-60 years). The clinical features, surgical treatment, and outcome are summarized in [Table - 1]. The main clinical presentations included headache, nausea, vomiting, recurrent seizures and focal neurological deficits. All the patients had associated hepatic involvement. Serological testing,(ELISA) was positive in five patients. On CT scan,AE lesions appeared as hypodense or isodense, masses. Calcification and surrounding edema were some of the common features seen. Contrast enhancement was observed within the inflammatory reaction around the lesion [Figure - 1] and [Figure - 2]. On MRI lesions were hypo- or isointnse on T1-weighted images and were of heterogeneous intensity on T2-weighted images with surrounding peri-lesional edema. Contrast enhancement was seen around the lesion in the inflammatory zone [Figure - 1] and [Figure - 2]. Surgical management All patients underwent operation by neurosurgery. According to the localization and volume of the lesion, different approaches were performed. Patients with lesions located in the cerebral hemispheres and with small volume, were allocated to massive resection group [Figure - 1], The bone flaps were always larger than the cross section of the mass and were opened with high speed drill slowly and carefully. The dura were incised without using electrocoagulation, and any adhesions between the dura and the cerebral pia mater were separated with sharp dissection. The cortex overlying the lesion had to be opened with only spatula retractors. The incision in the cortex was larger than the lesion. Once the lesions were displayed, thin strips of cotton were inserted between the lesion and the surrounding cerebral parenchyma. The brain tissue was gently separated from the mass with spatula retractors and aspirators. Four patients underwent radical gross resection. On the other hand, in patients with lesions located in the eloquent areas or with giant volume (the radical piecemeal resection group), debulking resection was performed. The third patient with lesion in the brainstem received radical piecemeal resection via the lateral suboccipital approach. The fifth patient with large mass located in the anterior cranial base in the midline area underwent entire debulking resection through a left frontal craniotomy [Figure - 2] and [Figure - 3]. Once lesions were exposed, thin strips of cotton were immediately inserted around the mass to protect the surrounding cerebral tissue. Then, microsurgery was performed by an internal debulking to gradually shrink the size of the mass until complete removal was achieved, according to interface between the normal brain tissue and lesion. After removal of these lesions, the spaces were carefully washed with 10% hypertonic saline solution repeatedly, and the whole cavity was filled with 0.9% saline solution. Cautious and leak tight closure of the dura was performed at the end of the procedure. Postoperatively, all patients received albendazole, 10 mg/kg body weight per day for lifetime as all the patients had associated inoperable liver involvement. Patients were given two weeks drug holiday for every four weeks of treatment. This was done to prevent cumulative drug toxicity if there is any. Outcome None of the patients had postoperative neurological worsening and all had improvement in the neurological deficits except the patient with blindness. At subsequent clinical evaluation, the patients remained neurologically asymptomatic except the patient with blindness. There were two deaths, one due to liver failure and the other related to untreated hydrocephalus at twelfth and eighteenth months of operation respectively. The remaining patients are back to their normal activity. Discussion In contrast to cysts echinococcosis (CE), the prevalence of cerebral AE in humans is quite rare. It is still the widespread, life-threatening parasitic infection prevalent in the Northern Hemisphere: Central Europe, Turkey, Russia, Japan, Alaska, North America, and China. [3],[9] Moreover, recent investigations have shown that some factors such as increasing prevalence of infection in fox population, the closer proximity between foxes and humans, and spillover of E. multilocularis infection from wild carnivores to domestic animals, might pose a considerable public health risk,. [1],[3] Intracranial AE account for ~1% of all cases of AE and is generally considered to be fatal. [9] The life cycle of E. Multilocularis involves carnivores: Fox, dog, wolf, and occasionally cat as definite hosts and herbivores: Rodent, pig, monkey, and hare,as intermediate hosts. [3],[9],[10] Humans are just incidental and aberrant intermediate hosts, who are usually infected by ingestion of ova from feces of carnivores via uncooked, contaminated green vegetables, water, and fruits .[3],[5],[9],[11] In the duodenum, these ova lose their membrane and the oncosphere is released from the keratinized embryophore and pass through the host's intestinal wall into the liver via the portal circulation. Although Reuter et al ., reported two cases with extrahepatic AE without liver involvement, the primary location of the AE, as a general rule, is always in the liver. [4],[12],[13] The capacity of the larva for exogenous proliferation enables it to initiate (usually via the bloodstream) the formation of distant metastases in lungs, brain, bones, kidneys, and other organs. [9] Cerebral metastases occurs in only 1% of the infected patients.[14] All the patients in this study had inoperable liver invasion, thus indicating that the cerebral AE in these patients was a secondary metastasis. In CE caused by E. grannulosus, the cyst wall is composed of two layers, the outer layer, laminated hyaline membrane (ectocyst) and an inner layer, germinal epithelium (endocyst). [15]. Where as human AE is a heterogeneous non-capsulated solid mass. It grows by exogenous and tumor-like proliferation and lacks a laminated membrane. The lack of laminated membrane allows the parasite to invade the host tissue in alveoli-like pattern. [16] In case of CE, in the inner germinal layer pullulation occurs always towards the cavity, producing scolices, daughter cysts, and ever grand-daughter cysts (in various stages of development). Thus while operating CE lesions, various techniques, including Dowling technique, should be employed for the safe delivery of the cerebral cysts without spilling their contents to avoid recurrence. Moreover, the wall is white, smooth, soft to touch, and elastic so that it can be totally removed through an incision smaller than its diameter without rupture. [17] These techniques allow the neurosurgeons to remove the CE lesion. However, the techniques may not be applicable for patients with cerebral AE lesion Studies have shown proliferation and metastases formation of larval E. muitilocularis in the natural intermediate host, Meriones unguiculatus. [18] However the pathogenesis of human cerebral metastases is not yet clear. Moreover, it is not clear whether or not the cerebral metastases contain protoscolex. [5],[6],[8],[12],[19] In the excised specimens of our patients, neither protoscolex nor germinative membranes could be identified [Figure - 4]. In the intermediate host the growth of protoscolex is quite rapid, 2 to 4 months, where as in human AE the formation and proliferation of protoscolex is very slow over 5 to 15 years. [4],[20] Some researchers feel that in human, the parasite does not form protoscolex and is made of a thin cuticle with nongerminative membrane.[21],[22] These observations suggests that incision of cerebral AE may not be the cause for larval distant metastasis. Two of our patients who had piecemeal resection, had no recurrence of the disease at 8 and 42 months of follow-up respectively and have resumed normal activities. We feel that piecemeal resection may be the procedure for lesions located in the eloquent areas. Of course, the optimum treatment of cerebral metastasis is surgical resection using radical procedures. But there is a risk of post-procedural major neurological deficits with radical procedure. In an attempt to balance the advantage of an aggressive surgical resection against the risk of associated significant morbidity and mortality, surgical procedures, in our opinion, have to be adapted to individual situation, such as stage of the disease, location and volume of the lesion, and other systemic factors. In case of small lesions located in the non-eloquent areas, radical massive resection should be the procedure of choice. The exact size and position of the lesion should be mapped on the surface of the scalp, and the bone flap should be larger than the cross section of the mass. And special attention should be taken on opening the bone flap as well as dura. Moreover, the incision of substantia corticalis must be larger than the lesion. However, it is impossible for the lesion to be removed when it is located in the brainstem and eloquent areas, without damaging the surrounding brain tissue. In these patients, piecemeal resection is the only option. Fortunately, they are really rare. To the best of our knowledge, no paper on piecemeal resection of cerebral AE has been reported so far. We performed piecemeal resection in two of the six patients with cerebral AE, and both the patients were followed up for 8 and 42 months, respectively. None of them had recurrence of the disease. We feel radical piecemeal resection along with albendazole therapy is probably the best treatment option for patients with large volume lesions and also for lesions located in the eloquent areas and brainstem. Long-term chemotherapy was essential component of treatment in our patients after radical resection of the cerebral lesions as they had inoperable hepatic primary infection. Albendazole is a parasitostatic agent against E. multilocularis metacestode, it can reduce the viability of protoscolices and cysts, and also its metabolite, albendazole sulfoxide, is active against the larval cestodes. [4],[23] Earlier experience with albendzole suggests that the drug is effective in killing E. multilocularis in few cases. [22] We preferred to use the interrupted-treatment regimen because of the hepatotoxicity of albendazole and also extensive hepatic involvement in these patients. In conclusion, human AE is a disease associated with serious complications and significant morbidity and mortality, especially cerebral AE. Even though surgical treatment for cerebral metastasis is palliative in patients with inoperable primary disease, it along with chemotherapy may relieve the symptoms and prolong the life. Radical massive resection is the optimal, but in certain cases, like brainstem lesions and lesions in the eloquent areas, where radical massive resection is not possible, radical piecemeal resection is a reasonable and effective alterative treatment strategy. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09045f1.jpg] [ni09045t1.jpg] [ni09045f3.jpg] [ni09045f4.jpg] [ni09045f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}