 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 2, March-April, 2009, pp. 188-190 Case Report Cerebral sinus thrombosis in a patient with active ulcerative colitis and double heterozygosity for Factor V Leiden and prothrombin gene mutations Fahri Yakaryilmaz, Sefa Guliter, Bulent Degertekin1 , Candan Tuncer 1 , Selahattin Unal 1 Department of Gastroenterology, Kirikkale University Faculty of Medicine, Kirikkale, and 1 Gazi University Faculty of Medicine, Ankara, Turkey Correspondence Address: Dr. Fahri Yakaryilmaz, 1.Sokak 8/13 Abidinpasa, 06620, Ankara - Turkey. fahriyy67@yahoo.com Date of Acceptance: 06-Mar-2009
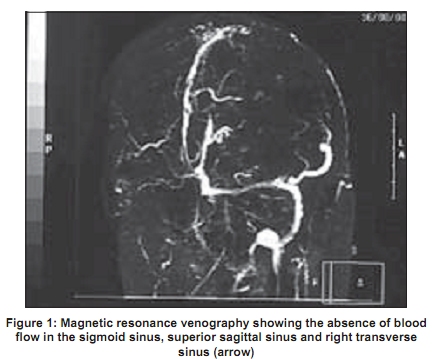
Code Number: ni09053 PMID: 19439852 DOI: 10.4103/0028-3886.51292 Abstract Inflammatory bowel diseases are associated with increased risk for thrombotic complications, In patients with ulcerative colitis (UC) cerebral sinus venous thrombosis (CSVT) is an extremely rare complication. We report a patient with active UC and CSVT. The patient was heterozygous for Factor V Leiden and G20210A prothrombin gene mutations without other identifiable precipitating factors. This patient highlights the need for investigating the patients with UC with thrombotic complications for other thrombophilic states.Keywords: Cerebral sinus thrombosis, Factor V Leiden mutation, ulcerative colitis Introduction Inflammatory bowel diseases (IBD) are associated with increased risk for thrombotic complications. The incidence of thromboembolic events in IBD is 13-64/1 000. [1] The reasons The reason for the increased risk of thrombotic complications is not clear. Cerebral sinus venous thrombosis (CSVT) is a rare complication in IBD and till date only 25 cases have been documented. The possible risk factors include the prothrombotic states associated with IBD and corticosteroid usage. [2] Heparin has been used successfully to treat thrombi in the small vessels of mucosa and submucosa in patients with IBD. [3],[4] We report a thrombotic complication, CSVT, in a young patient with ulcerative colitis (UC) who was hetrozygous for Factor V Leiden (FVL) and prothrombin gene mutations. Case Report A 23-year-old woman a known case of UC for the past two years, was admitted for recurrence of UC. The diagnostic evaluation at the initial admission included colonoscopy and biopsy. Colonoscopy cofirmed pancolitis with pseudopolyps (endoscopic activity score = 10) and biopsy revealed a histologic picture consistent with acute UC. Since the diagnosis she has been treated with mesalazine irregularly. She was a non-smoker and had not used oral contraceptive pills. At current admission, her symptoms were abdominal pain, bloody diarrhea (a total of 10 to 15 motions with blood and mucous), weight loss (8 kg in the past two months), headache, nausea, left-sided hemiparesis. Physical examination revealed body temperature of 37°C, blood pressure of 100/70mmHg and pulse of 98 beats/min. Examination of heart and lungs was normal. She was pale and had Grade 1/4 edema in lower extremities. Neurological examination revealed left hemiplegia, motor power upper limbs 0/5 and lower limbs 0-2/5. Deep tendon reflexes on the left side were brisk with extensor plantar response. There were no other neurological deficits. Laboratory evaluation showed an erythrocyte sedimentation rate of 85 mm/h, hemoglobin of 9.5 g/dL, white blood cell count of 8.800/mm 3 , platelet count of 602.000/mm 3 , mean corpuscular volume of 85fl, C-reactive protein of 9.6mg/dL, and serum albumin of 2.2g/dL. Serum electrolytes, creatinine and blood urea were normal. Serum vitamin B12 and folic acid, fibrinogen and homocysteine were within normal limits. Coagulation profile: Prothrombin time 12.6 s, partial thromboplastin time 34.2 s, protein C 43%, protein S 30% and antithrombin III 102%, and activated protein C (APC) ratio 0.52. Other laboratory data including anticardiolipin antibodies and lupus anticoagulant were negative; FVL and prothrombin gene mutations were heterozygous positive, and MTHFR mutation was negative. A post contrast computed tomography (CT) scan showed right occipito-parietal non-hemorrhagic lesions. Magnetic resonance imaging (MRI) of the brain revealed right occipito-parietal multiple non-hemorrhagic lesions. MRI selected angiography demonstrated thrombosis of sigmoid sinus, superior sagittal sinus and right transverse sinus thrombosis [Figure - 1]. Treatment with prednisone (60mg/day) and heparin (15.000 U/day) iv was started. The headache and left motor deficit improved and the phase contrast MRI angiography of the sigmoid sinus, superior sagittal sinus and right transverse sinus was almost normal four weeks after the initiation of the treatment. She was put on maintenance treatment with warfarin (dose adjusted according to INR), prednisone (20 mg) p.o, and azathioprine (100mg) p.o. Discussion Thrombotic complications are recognized but uncommon complications of IBD and occur in 1.3-6.4% of all cases of IBD. The coagulation abnormalities associated with active IBD include elevated levels of Factors V and VII and fibrinogen and decreased levels of antithrombin III. Other factors that may contribute to thrombosis include dehydration and quantitative and qualitative platelet disorders. [1] Hereditary and acquired factors that have been shown to play a role in the pathogenesis of the hypercoagulable state: Protein C and protein S deficiency, APC resistance, FVL gene mutation, prothrombin gene mutation, hyperhomocysteinemia and antiphospholipid antibodies. [2] Our patient was heterozygous for FVL and prothrombin gene mutations and workup for the thrombophilic states associated with IBD was negative. In the study by Liebman et al ., [3] 36% of patients of IBD with thrombotic complications had FVL mutations whereas it was only 4% in patients with no thrombotic complications. [3] Vecchi et al ., did not find any correlation between hereditary conditions predisposing to thrombosis such as FVL mutation, prothrombin gene mutation, MTHFR mutation, proteins C and S, antithrombin III deficiencies and IBD. [2] Turri et al ., [4] investigated the prothrombin gene and FVL mutations in patients with IBE with and without a history of thrombotic complications and also in healthy subjects. In this study none of the patients with a history of thrombotic complications had mutations and 2.2% of patients without a history of thrombotic complications were heterozygous for FVL mutation. Srivastava et al., [5] reported a 29-year-old male patients with UC who developed superior sagittal, left lateral and sigmoid sinus thrombosis. This patient had normal coagulation profile and they have not investigated for thrombosis associated gene mutations. FVL and prothrombin G20282A gene mutations were found to be increased in patients with IBD with a history of thrombotic complications compared to patients with IBD without a history of thrombotic complications; however, no difference was observed between the patients without thromboembotic complications and the normal population. [6] Umit and colleagues [7] reported CSVT in a 53-year male with active UC who was heterozygous to FVL mutation. The patient reported by Bιchade et al., [8] developed CSVT during the inactive phase of UC while the steroid dose was being tappered off and the workup for inherited thrombophilia was negative. In conclusion, we described a patient with UC and cerebral sinus thrombosis who was detected to have both FVL and heterozygote prothrombin gene mutations, and whose symptoms of UC and sinus thrombosis improved after treatment with prednisone, azathioprine and anticoagulant therapy. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09053f1.jpg] |
| |||||||||


{kind=link}