 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 2, March-April, 2009, pp. 203-205 Case Report Adult medulloblastoma mimicking Lhermitte-Duclos disease: Can diffusion weighted imaging help? Puneet Mittal, Kamini Gupta, Kavita Saggar, Supreet Kaur Department of Radiodiagnosis, Dayanand Medical College and Hospital, Ludhiana, Punjab, India Correspondence Address: Dr. Puneet Mittal, Department of Radiodiagnosis, Dayanand Medical College & Hospital, Tagore Nagar, Civil Lines, Ludhiana, Punjab - 141 001, India. drpuneetmittal@gmail.com Date of Acceptance: 31-Mar-2009
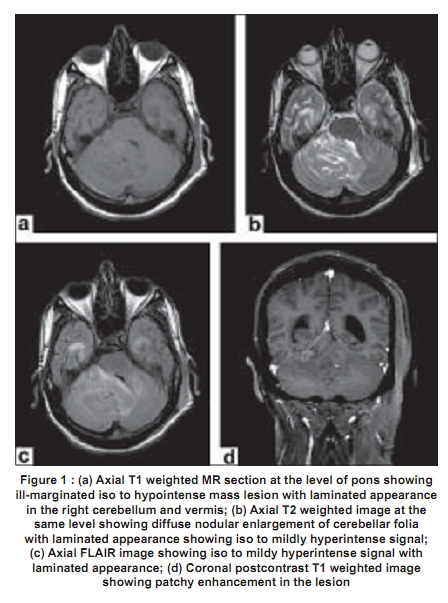
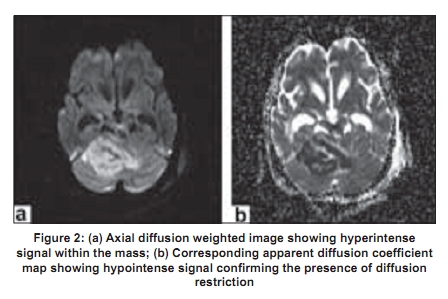
Code Number: ni09058 PMID: 19439857 DOI: 10.4103/0028-3886.51297 Abstract Lhermitte-Duclos disease, also known as dysplastic cerebellar gangliocytoma, is a rare cerebellar benign tumor with characteristic appearance of thickened cerebellar folia giving a laminated or striated appearance, quite diagnostic of the condition. We had seen a patient with medulloblastoma with imaging findings suspicious for thickened cerebellar folia reminiscent of Lhermitte-Duclos disease. However, it showed patchy contrast enhancement and restricted diffusion on diffusion-weighted imaging, which are not typically associated with Lhermitte-Duclos disease. Presence of restricted diffusion proved to be a useful diagnostic feature for differentiation between the two lesions. This patient highlights the importance of obtaining all the MR imaging sequences in suspected Lhermitte-Duclos disease and histological diagnosis if there is doubt.Keywords: Diffusion, folia, gangliocytoma, Lhermitte-Duclos, medulloblastoma Introduction Medulloblastoma accounts for ~1% of adult brain tumors and 14-35% of medulloblastomas occurs in adults and show atypical features. [1],[2],[3] Lhermitte-Duclos disease is a rare entity and about 220 cases have been reported till 2006. [4] We present an adult patient with medulloblastoma with suspicion of abnormal folia thickening masquerading as Lhermitte-Duclos disease. Our review of literature showed only two such case reports of medulloblastoma in children. [5],[6] Both of them were misdiagnosed as Lhermitte-Duclos disease. Case Report A 19-year-old male patient presented with headache, projectile vomiting, and weight loss of two months duration. Two days prior to the contrast magnetic resonance imaging (MRI) study, a ventriculoperitoneal (VP) shunt was placed for obstructive hydrocephalus. The contrast MRI revealed an ill-defined right cerebellar mass with suspicion of thickened cerebellar folia giving a striated appearance involving the vermis and middle cerebellar peduncle causing mass effect on the brainstem and fourth ventricle and transtentorial herniation. The lesion was hypointense on T1-weighted (T1W) images [Figure 1a], and iso to mildly hyperintense on T2-weighted (T2W) [Figure 1b] and fluid attenuation and inversion recovery (FLAIR) images [Figure 1c]. On postcontrast images, mild patchy enhancement was seen [Figure 1d]. The mass showed restricted diffusion on diffusion weighted (DW)/apparent diffusion coefficient (ADC) images [Figure 2a,b]. Calculated ADC value in the region of the mass was 303 µm 2 /s while the ADC value in the adjacent normal cerebellar white matter was 707 µm 2 /s. Appearance of thickened folia in this patient suggested the diagnostic possiblity of Lhermitte-Duclos disease. However, contrast enhancement and restricted diffusion were atypical features. Possibilities of Lhermitte-Duclos disease and medulloblastoma were considered. On surgical pathology, it was proven to be medulloblastoma. Discussion Medulloblastoma is a malignant primitive neuroectodermal tumor. Although it is generally considered to be a childhood tumor, a significant number of cases (14-35%) occur in adults with maximum incidence between 15 and 19 years of age. [1],[2],[3] Medulloblastoma is thought to arise from primitive neuroectodermal cells found in the floor of the fourth ventricle. These cells migrate upward and laterally to form the external granular layer. Medulloblastoma can develop anywhere along this path. Furthermore, the cells migrate more laterally with increasing age, this may explain the midline location of these tumors in children and the lateral location in adults. [7],[8] The cerebellar location of medulloblastoma is between 50% and 63%. [7],[9] The classical imaging appearance of medulloblastoma is that of a homogeneous midline vermian mass which shows uniform enhancement without any necrosis or cystic areas. While these features are seen more commonly in children, in adult tumor tends to be more heterogenous with cystic and necrotic areas. Tumor tends to be isointense on T2W images. This feature is attributed to hypercellularity of the tumor and also desmoplastic medulloblastomas.being more common in adults. In adults contrast enhancement is variable. [8],[10] Medulloblastomas, like all other primitive neuroectodermal tumors, are hypercellular tumors. These are associated with less amount of extracellular water. This histological pattern is responsible for the restricted diffusion seen in medulloblastoma and could be potentially useful in differentiating it from other tumors. [10],[11] Lhermitte-Duclos disease, also known as dysplastic cerebellar gangliocytoma, is an uncommon tumor of uncertain origin, commonly seen in adults. It is classified as World Health Organization (WHO) grade I tumor. [12] MRI is the imaging modality of choice. Typically the cerebellar hemispheric mass does not enhance on contrast and is hypointense on T1W and hyperintense on T2W images with characteristic laminated appearance due to abnormal thickening of cerebellar folia. It is usually unilateral but can extend into the vermis. [13],[14] Although it is usually an avascular lesion, few cases with contrast enhancement have been reported. [15],[16] On diffusion-weighted imaging, Lhermitte-Duclos disease shows increased signal intensity due to T2 shine-through effect rather than restricted diffusion as reflected by lack of hypointensity on ADC mapping. [13],[17],[18] In our case, the findings closely resembled that of Lhermitte-Duclos disease with thickened folia. Mild contrast enhancement has also been reported in Lhermitte-Duclos disease. Presence of restricted diffusion in our case led us to suspect the diagnosis of medulloblastoma. In the two previous such cases the initial diagnosis was Lhermitte-Duclos disease. The patient reported by Someshwar et al ., [3] had restricted diffusion, however this finding was not considered in the diagnosis. MR spectroscopy can be useful in the differential diagnosis. Medulloblastoma shows typical characteristics of a mitotic lesion with increased choline (Cho)/creatine (Cr) and Cho/N-Acetyl Aspartate (NAA) ratios. [19] On the other hand, Lhermitte-Duclos disease shows spectroscopic findings of a hamartomatous lesion., decreased NAA/Cr ratios and no increase in Cho/Cr ratio. [17],[20] Both medulloblastoma and Lhermitte-Duclos disease can show increased perfusion parameters on MR perfusion imaging. [20],[21] This case highlights the importance of doing all the MRI sequences in suspected cases of Lhermitte-Duclos disease. Presence of restricted diffusion might question the diagnosis of Lhermitte-Duclos disease. Such cases should be considered for early histological diagnosis, as management of Lhermitte-Duclos disease and medulloblastoma is different and misdiagnosis can be potentially harmful. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09058f1.jpg] [ni09058f2.jpg] |
| |||||||||


{kind=link}
{kind=link}