 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 2, March-April, 2009, pp. 206-207 Case Report Ondine's curse after brainstem infarction José Luiz Pedroso, Robson Fantinato Baiense, Ana Paula Scalzaretto, Pedro Braga Neto, Aécio Flávio Teixeira de Góis, Maria Elisabeth Ferraz Department of Neurology and Neurosurgery, Federal University of São Paulo, São Paulo, Brazil Correspondence Address: Dr. José Luiz Pedroso, Pedro de Toledo Street, 544/206, São Paulo, São Paulo, Brazil. zeluizpedroso@yahoo.com.br Date of Acceptance: 31-Mar-2009
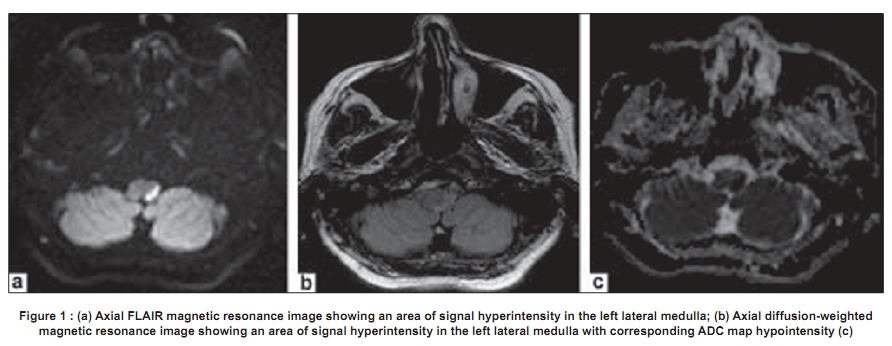
Code Number: ni09059 PMID: 19439858 DOI: 10.4103/0028-3886.51298 Abstract This report describes a rare case of acquired Ondine's curse. The patient developed central sleep apnea syndrome named Ondine's curse after a brainstem infarction. Lesions involving the descending medullocervical pathways that subserve automatic breathing can result in this syndrome.Keywords: Brainstem infarction, central sleep apnea, ondine's curse Introduction Ondine's curse is a rare and severe condition and is characterized by loss of automatic respiration during sleep and preserved voluntary breathing. [1],[2] The term stems from a mythological European tradition in which Ondine, a water nymph, condemns her unfaithful lover to loss of all movements and functions that do not require conscious will. A similar situation occurs in Ondine's curse. Patients with this condition are compelled to remain awake in the nights lest they stop breathing and they need night-time mechanical ventilation to survive. [1] In 1962, Severinghaus and Mitchell [2] were the first to use the term 'Ondine's curse' for patients who developed long periods of apnea but would breath on command. The diagnostic criteria for Ondine's curse are not well established. The proposed criteria include: Hypercapnia during non-REM sleep; normal PO 2 (arterial blood gas, (ABG)) during voluntary breathing when awake; alveolar hypoventilation during sleep; and exclusion of pulmonary diseases. [3] We report a patient with Ondine's curse following left lateral medullary infarction, Wallenberg's syndrome. Case Report A 79-year-old white woman presented to the hospital with sudden onset of dizziness, loss of balance, and dysarthria of one hour duration. She was a known case of hypertension. On examination, she was awake and was slurred and dysphonic. She had left side palatal weakness, Horner's syndrome and limb incoordination and also diminished sensations in the right half of the body. Brain magnetic resonance imaging (MRI) revealed hyperintense signal in the left lateral medulla [Figure - 1]. Electrocardiogram, echocardiogram, and chest radiograph were normal. Other laboratory tests during the first week of admission were within normal limits. Cervical Doppler studies showed diffuse atheromatous changes and flow velocity in the left vertebral artery was at the lower limit of normal. MR-agniography was normal. She was prescribed aspirin. During her stay in the intensive care unit (ICU), she had many episodes of sudden apnea, especially during the nights. She developed aspiration pneumonia. The patient had emergency intubation and mechanical ventilation. ABG, when the patient was on pressure support ventilation, showed persistent hypercapnia during sleep (PCO 2 between 80 and 90 and PO 2 under 65) and the gases were normal when she was awake. She could not be weaned off from ventilation because of frequent apnic episodes. She received acetazolamide, levothyroxin, and clomipramine with no benefit. She had prolonged episodes of apnea during the ICU stay, more so when support pressure ventilation was tried. Diaphragmatic pacemaker was considered but could not be done as there is no trained professional to do the procedure at our institute. She died two months postadmission following nosocomial pneumonia, sepsis, and chock. Discussion The patient fulfilled most of the diagnostic criteria for Ondine's curse. Ondine syndrome is commonly described as a congenital central hypoventilation. However, cases of acquired Ondine's curse have been reported.[2],[3],[4] Lesions selectively involving the ventrolateral descending medullocervical pathways that subserve automatic breathing can result in Ondine's curse. [1] There are number of causes that can cause the syndrome: Brainstem infarction, hemorrhage, encephalitis, Leigh syndrome, traumatic Duret hemorrhage, medullary tumors, mitochondrial disease, degenerative diseases (e.g. multisystem atrophy), demyelinating diseases (e.g. multiple sclerosis), and nonspecific anoxic-ischemic insult. [4] Pharmacological treatment seems not to be of benefit in this condition. Medications tried included acetazolamide, levothyroxin, and clomipramine. None of these medications was of benefit in our patient. Spontaneous recovery has been documented. But most patients need mechanical ventilation for variable periods. Diaphragmatic pacing may be considered in patients with prolonged periods of mechanical ventilation and frequent episodes of apnea. [5] The prognosis of the disease is variable, depending on the location of the lesion and the nature of the pathology. Recovery, although frequent, is usually unpredictable. [6] Death usually occurs during sleep, probably due to total apnea. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09059f1.jpg] |
| |||||||||

{kind=link}