 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 2, March-April, 2009, pp. 216-217 Letter To Editor Unusual cutaneous reaction with sodium valproate S. Roy, Deepak Goel 1 Department of Dermatology and Neurology1 , Himalayan Institute of Medical Sciences, Swami Ram Nagar, Dehradun (UT), India. Correspondence Address: Department of Neurology, Himalayan Institute of Medical Sciences, Swami Ram Nagar, Dehradun (UT), India goeld007in@yahoo.co.in Date of Acceptance: 31-Mar-2009
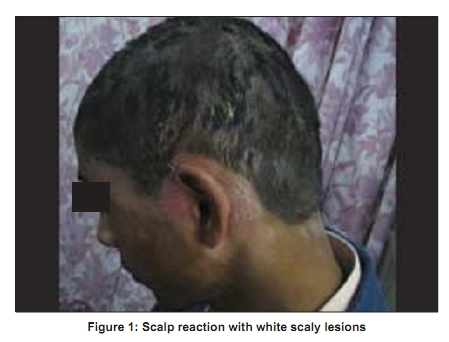
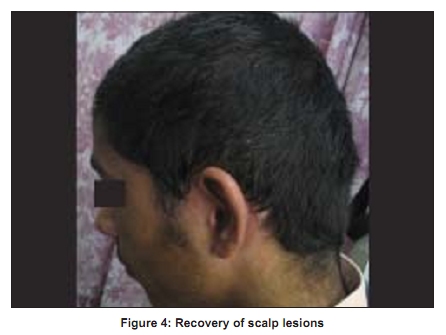
Code Number: ni09063 PMID: 19439862 DOI: 10.4103/0028-3886.51302 Sir Cutaneous eruptions are one of the most common type of drug-related adverse reactions and accounted for 2-3% in hospital-based series . [1].[2] About 10% of patients receiving antiepileptic drug therapy develop skin allergy. [1] Among the AEDs, sodium valproate is relatively free from skin allergy. This report describe a patient who developed sevee psoriasiform eruption with sodium valproate. A 14 years boy was started on sodium valproate (extended release preparation) 500mg per day for recurrent left focal onset complex partial seizures following traumatic brain injury. Four months after starting sodium valproate he developed hair fall with white scaly scalp lesions. Gradually these lesions enlarged involving almost entire head and periauricular areas [Figure - 1]. He also developed multiple discrete and confluent white scaly lesions with raised erythematous margins over the trunk, chest, and limbs [Figure - 2]. The morphology of the lesions was suggestive of psoriasoform eruption. Histology of the skin biopsy showed hyperkeratosis, parakeratosis, loss of granular layer, irregular acanthosis of the epidermis, and a perivascular infiltrate composed of mononuclear cells in the upper dermis. Patient was discontinued of valproate and was started on oxcarbazepine. The eruption completely disappeared in four months [Figure - 3] and [Figure - 4]. At 12 months follow up he was absolutely normal without any relapse of skin lesions. Development of psoriasiform eruption with the initiation of valproate and subsequent remission of the lesions with the discontinuation of the drug and subsequent course clearly suggests a causal relation between valproate and skin lesions. Various types of drug-related cutaneous eruptions include: Maculopapular rash, fixed drug eruption (FDE), erythema multiforme (EM), toxic epidermal necrolysis (TEN), Stevens-Johnson syndrome (SJS), urticaria, and erythroderma. [1] Maculopapular rash is the most common skin lesion with AEDs. The serious skin allergies include SJS and TEN. Skin allergies have been described more often in patients receiving carbamazepine, phenytoin and lamotrigine. [2] Cutaneous eruptions are least with valproate compounds. Review of English literature showed only report of two cases of psoriasiform eruption with valproate. [3],[4] Drug treatment may result in exacerbation of pre-existing psoriasis, can induce psoriatic lesions on clinically uninvolved skin in patients with psoriasis, or can precipitate the disease in predisposed individuals. [5] Our patient had no past or family history of psoriasis and no relapse of lesions at one year of follow up, thus suggesting that the psoriasiform eruption in him were probably related to valproate treatment. The knowledge of the drugs that may induce, trigger, or exacerbate psoriasis, is of importance in clinical practice. The drugs that may induce psoriasis include lithium, beta-adrenergic antagonists, antimalarial, non-steroidal anti-inflammatory drugs (NSAIDs) and rarely tetracycline. [6] To this list we should add valproate and valproate should be used with caution in individuals with pre-existing psoriasis. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09063f1.jpg] [ni09063f4.jpg] [ni09063f3.jpg] [ni09063f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}