 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 2, March-April, 2009, pp. 221-222 Letter To Editor Spontaneous thoracic spinal cord herniation presenting as tethered cord syndrome Narayanam A. Sai Kiran, Sandeep Vaishya, Manish K. Kasliwal, Shashank S. Kale, Bhavani S. Sharma Department of Neurosurgery, All India Institute of Medical Sciences, New Delhi, India. Correspondence Address: Department of Neurosurgery, All India Institute of Medical Sciences, New Delhi, India. kalesaiaiims@yahoo.com Date of Acceptance: 12-Mar-2009
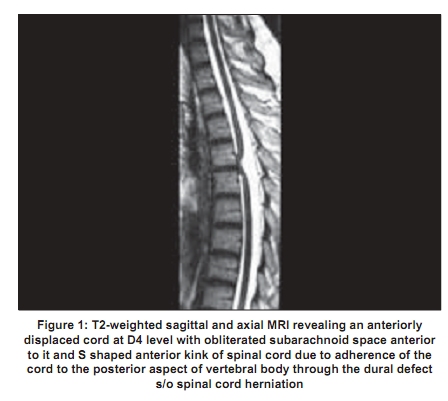
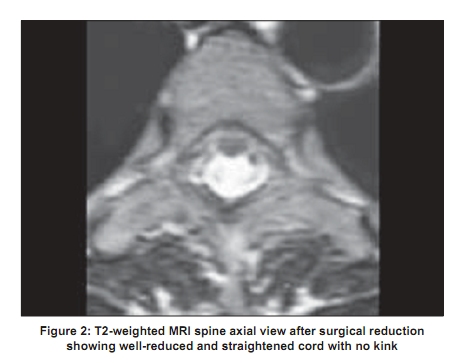
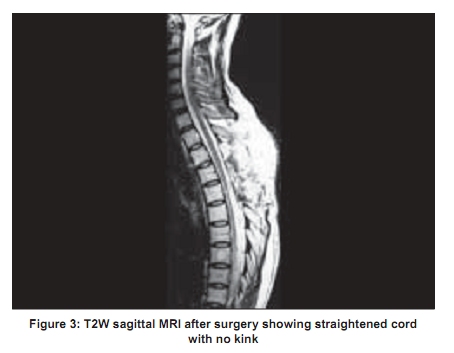
Code Number: ni09067 PMID: 19439866 DOI: 10.4103/0028-3886.51306 Sir, A 36-year-old female presented with dysesthetic pain below the costal margin associated with progressive weakness of both lower limbs and wasting of right thigh muscles of one and half year duration and symptoms suggestive of upper motor neuron type of bladder of three months duration. Neurological examination revealed pyramidal signs in both the lower limbs, spasticity in the left lower limb and bilateral plantar extensor response. In addition she had wasting of right thigh muscles. Motor power was 4/5 in the left lower limb and 0/5 in the right lower limb. Magnetic resonance imaging (MRI) of the spine [Figure - 1] revealed an anteriorly displaced cord at D4 level with obliteration of subarachnoid space and "S" shaped anterior kink of the spinal cord due to adherence of the cord to the posterior aspect of vertebral body through the dural defect. Patient underwent D3-D5 laminectomy and reduction of the herniation. At operation nerve roots were matted with thickened arachnoid. Cord was anteriorly adherent at D4 level. There was kinking and lateral rotation of the cord. Cord herniation through the small dural defect was identified and reduction was done by microsurgery and the defect was closed with teflon graft. Patient had good recovery and was able to ambulate with support. Postoperative MRI revealed good reduction of the herniation and restoration of normal anatomy [Figure - 2]. Idiopathic anterior spinal cord herniation (SCH) is a rare cause of thoracic myelopathy. [1],[3],[4],[5] Significant delay between the onset of symptoms and surgery is probably due to two factors: Rarity of the lesion and the entity often being misdiagnosed initially as posterior intradural arachnoid cyst. [2] The mechanisms for the dural defect is still uncertain. The proposed mechanisms include: Minor trauma, duplication of the dura, rupture from prolapsed disc, congenital dural defect, and pressure erosion from the physiologically closely applied midthoracic cord to anterior dura. [2],[3],[4] Regardless of the mechanism, progressive herniation of the cord occurs as a result of of cerebrospinal fluid pulsations as well as negative epidural pressure. [2],[3] This results in progressive neurological symptoms. In addition tethering of the cord restricts the normal movements of spinal cord associated with flexion of the spine. [6] The resultant traction of the cord may also be a contributory factor for the progressive neurological deficits. Other factors that may contribute to progressive myelopathy include distortion of the cord and cord ischemia. Though spontaneous spinal cord herniation is a very rare entity, early recognition and timely intervention can lead to good neurological recovery.[Figure - 3] References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09067f3.jpg] [ni09067f1.jpg] [ni09067f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}