 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 2, March-April, 2009, pp. 229-230 Neuroimage Extensive gliosis in the wall of cervico-dorsal syrinx masquerading intramedullary tumor Amit Agrawal, Rajesh Dulani 1 , Arvind Bhake2 , Kishore M. Hiwale2 , Anita Mahadevan3 , S. K. Shankar 3 Departments of Surgery, 1 Orthopedics and 2 Pathology, Datta Meghe Institute of Medical Sciences, Sawangi (Meghe), Wardha, 3 Department of Neuropathology, National Institute of Mental Health and Neurosciences, Bangalore, India Correspondence Address: Dr. Amit Agrawal, Clinical and Administrative Head, Division of Neurosurgery, Datta Meghe Institute of Medical Sciences, Sawangi (Meghe), Wardha - 442 004, Maharashtra, India. dramitagrawal@gmail.com Date of Acceptance: 26-Jan-2009
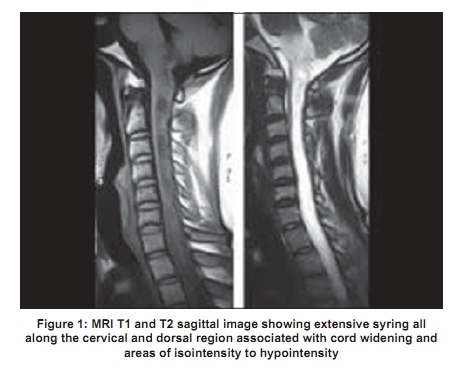
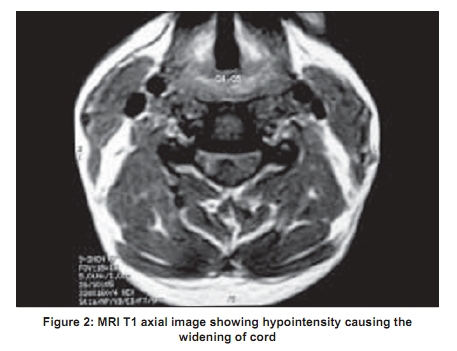
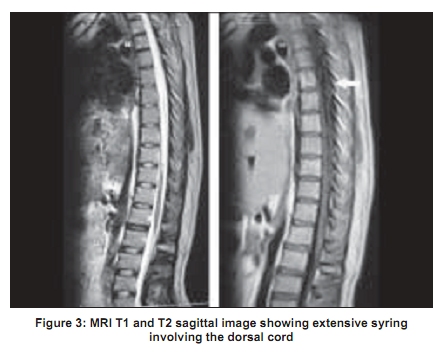
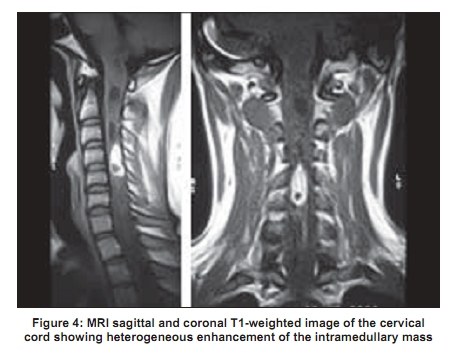
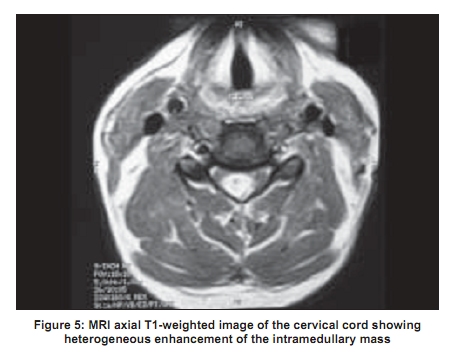
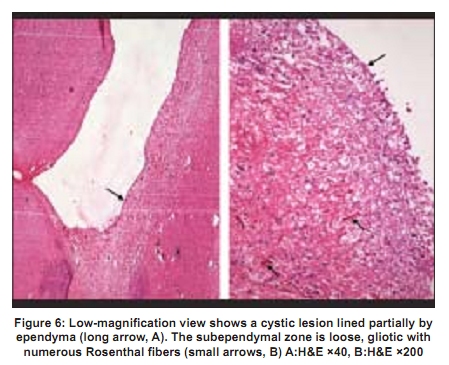
Code Number: ni09073 PMID: 19439872 DOI: 10.4103/0028-3886.51312 A 32-year-old gentleman presented with weakness, tingling, and numbness of all the four limbs for one month. He was operated for hydatid liver four years back. There was grade 4/5 weakness of all the four limbs with spasticity in the lower limbs and decreased sensation below C4. Reflexes were exaggerated in lower limbs and sluggish in upper limbs. Magnetic resonance imaging (MRI) showed extensive cervico-dorsal syrinx [Figure - 1],[Figure - 2],[Figure - 3]. Gadolinium-enhanced images showed heteroge-neously enhancing cystic lesion at C4-5 [Figure - 4] and [Figure - 5]. At surgery a gray-yellow, firm, well-defined mass was resected. The patient deteriorated by two grades immediate postoperatively, but recovered thereafter. Histopathological examination showed cystic lesion lined by ependymal lining. The wall showed dense fibrillary isomorphic gliosis entrapping anterior horn cells with numerous Rosenthal fibres [Figure - 6]. No immature neuronal or glial elements were found. Characteristic biphasic pattern of a pilocytic astrocytoma with loose microcystic zones and eosinophillic granular bodies was not evident. The findings were suggestive of extensive gliosis in the wall of the syrinx [Figure - 6]. In idiopathic syringomyelia, there are longitudinally oriented cavities with surrounding gliosis, attributed to arachnoiditis without any evidence of a true neoplasm.[1],[2] As in the present case clinically and radiologically these lesions can masquerade as intramedullary tumor with syringomyelia. [1],[2] The leading edge of the syrinx cavity dissects along longitudinal tissue planes leading to hypertrophic and hyperplastic gliotic changes. [1],[3] Gliosis is proportional not only to the age of the lesion but to the severity of the forces acting upon the walls, [4] and can be seen as circumferential bands producing "beaded" appearance. [3],[5] Gliosis is commonly associated with syringomyelia [1],[2],[5] and on MRI can show heterogeneous contrast enhancement. [2] References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09073f3.jpg] [ni09073f2.jpg] [ni09073f6.jpg] [ni09073f4.jpg] [ni09073f5.jpg] [ni09073f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}