 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
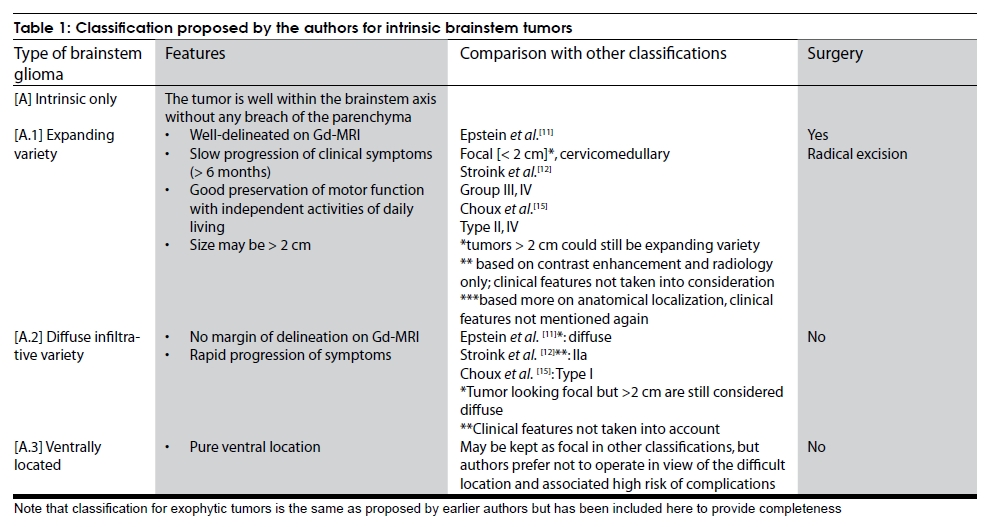
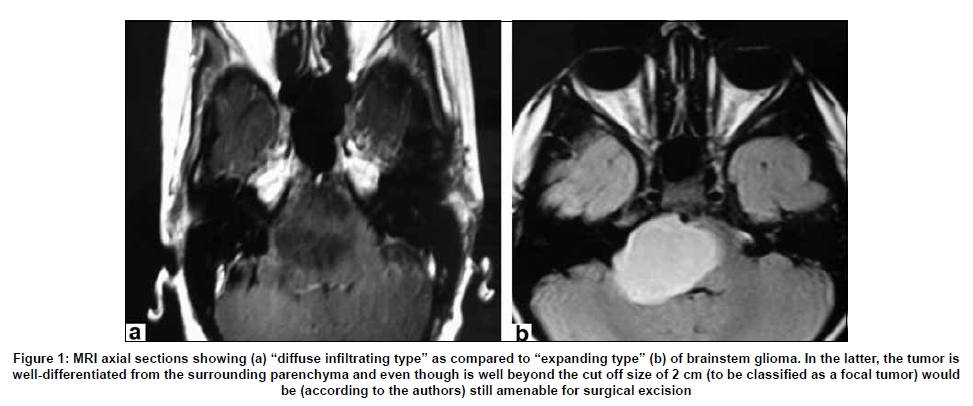
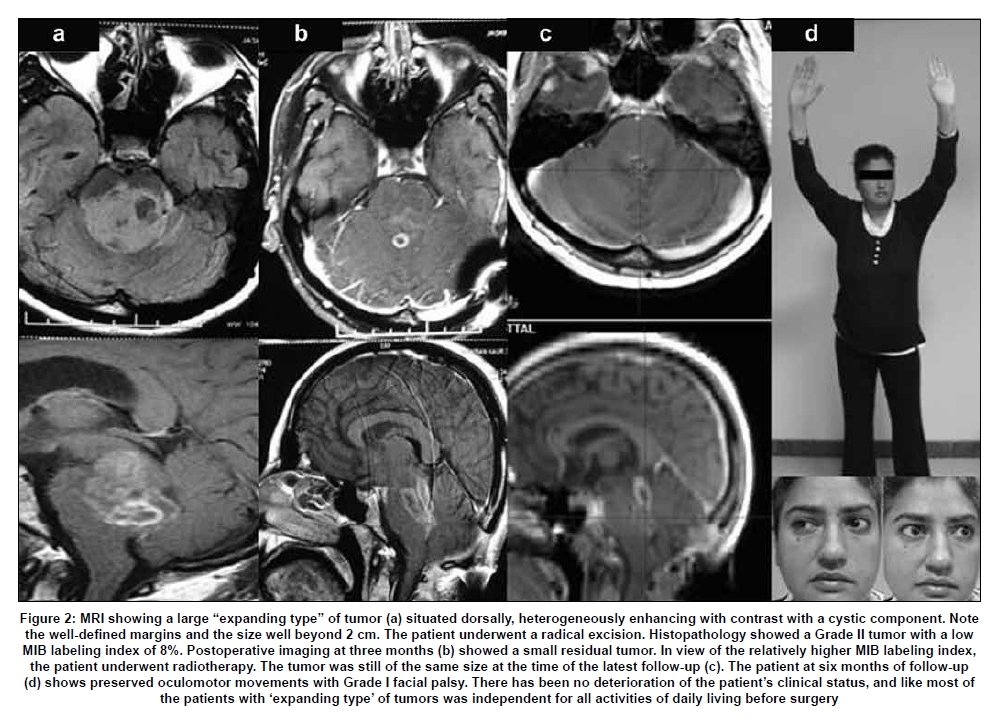
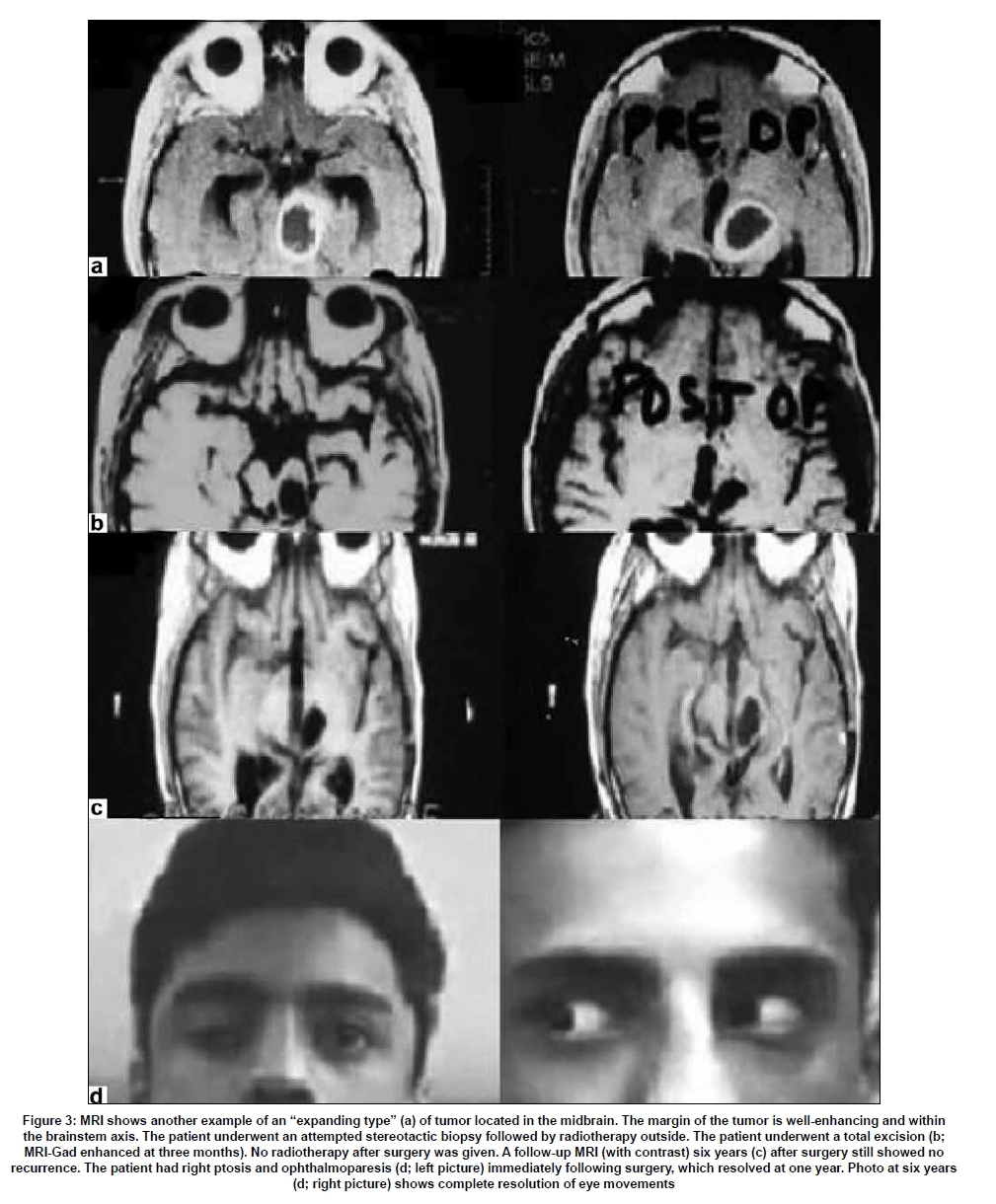
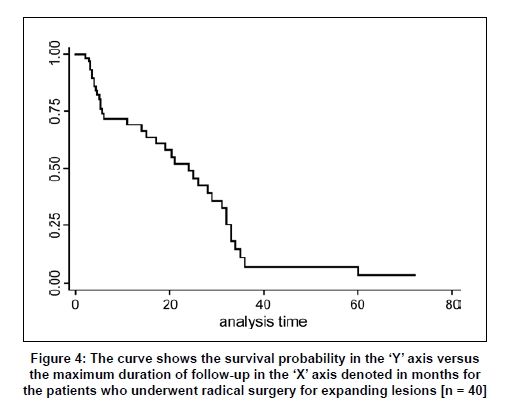
Neurology India, Vol. 57, No. 3, May-June, 2009, pp. 274-281 Original Article Surgical considerations for 'intrinsic' brainstem gliomas: Proposal of a modification in classification V. S. Mehta, P. S. Chandra1 , Pankaj Kumar Singh1 , Ajay Garg2 , G. K. Rath3 Paras Hospitals, Gurgaon, Departments of 1 Neurosurgery, 2 Neuroradiology and 3 Radiotherapy, All India Institute of Medical Sciences, New Delhi, India Date of Acceptance: 26-Apr-2009 Code Number: ni09082 PMID: 19587467 DOI: 10.4103/0028-3886.53272 Abstract Background: Brainstem gliomas are highly heterogeneous tumors both in their clinical manifestation and in their pathology. Despite significant advances in the surgery for brainstem gliomas many aspects of this pathology are still unclear Objective: To evaluate the clinical, radiological and surgical outcome of 40 focal 'intrinsic' brainstem gliomas and propose a surgical strategy-oriented classification. Materials and Methods: A total of 40 focal 'intrinsic' ("expanding variety") tumors have been operated over a period of 8.5-years (January 1998-June 2007). Our criteria included patients with (1) well-defined gadolinium enhancing tumor; (2) relatively long duration of symptoms (> six months) and (3) good neurological functional status and independent for all activities of daily living. The cutoff size of 2 cm was not rigidly adhered to. Results: The 'intrinsic' brainstem tumors were classified into three types: Expanding, diffuse infiltrative and pure ventral varieties. Only patients with expanding variety of brainstem gliomas were subjected to surgery, mean age 19.2 years (range 4-55 years) and male to female ration mean: 3:2). The tumor location included pons (n=19), midbrain (n=13) and medulla (n=8). Surgical approaches included midline suboccipital (n=28), retromastoid (n=7), subtemporal (n=3) and supracerebellar-infratentorial (n=2). Thirty-two cases with 'diffuse infiltrative' and 'pure ventral' variety were given radiotherapy only. Histology pathology revealed pilocytic variety (n=10), Grade II (n=17) and Grade III (n=13). There was one death in the surgical series (due to aspiration). Complications included meningitis (n=2), wound infection (n=1), chest infection (n=5) and transient mutism (n=1). Follow-up ranged from 3-68 months. Overall, 36 improved /remained same and three worsened in their clinical status at the time of discharge. Conclusion: The surgical management of intrinsic brainstem tumors presents a surgical challenge; radical excision yielded a good outcome in the majority of cases. The authors propose a classification system for 'intrinsic' brainstem tumors for defining surgical strategy.Keywords: Brainstem, focal, gliomas, intrinsic Introduction Brainstem gliomas are highly heterogeneous tumors both in their clinical manifestation and in their pathology. They occur commonly in children, accounting for 10-20% of all central nervous system tumors and they may occur in adults too. [1] The term "brainstem glioma" is an imprecise descriptive word and suggests that the behavior of all such tumors is likely to be the same, which may not be true. Prognosis in these tumors may be directly related to grade of tumor and location. [1],[2],[3],[4],[5],[6],[7] Amongst all the types of brainstem gliomas, there has been relatively sparse description in the literature on the "intrinsic" variety, [3],[4],[5],[6],[7],[8],[9],[10] particularly those falling under WHO Grade I category, with well-defined focal pathology but within the brainstem axis i.e. "intrinsic". While these tumors present a surgical challenge, a radical removal, if not followed by any significant complications, may yield a good long-term outcome in the majority of cases. Despite significant advances in the surgery for brainstem gliomas many aspects of this pathology are still unclear: (1) Inspite of several proposed classifications mostly based on anatomical location, [5],[11],[12],[13],[14] the surgical plan is still difficult to decide in many cases. In this aspect the classification proposed by Choux et al. , [15] perhaps comes closest in defining a surgical plan; (2) The difference between diffuse and large focal intrinsic brainstem gliomas is not clearly distinguished in most of the classifications. Thus sometimes it is possible that a large focal intrinsic benign tumor may not be subjected to surgery and sent for radiotherapy directly; (3) It is usually not possible radiologically to determine whether the tumor is benign or malignant. A stereotactic biopsy too may have limitation, it may pick up a benign portion of a malignant tumorn or vice versa. Thus a more important approach would be to try and remove the tumor as radically as possible provided the radiological image reveals such an opportunity, preferably by surgeon who has sufficient experience in this area. The aim of this study was to review our experience in the surgery for ′intrinsic′ brainstem gliomas, all operated by a single senior experienced surgeon and examine the outcome in relation to the surgical approach and nature of the imaging and to propose a simple working classification for defining surgical strategy. Materials and Methods Only the ′intrinsic′ brainstem tumors were included in this retrospective study. By the term ′intrinsic′ the authors indicate that the tumor is still contained within the boundaries of the brainstem parenchyma without an exophytic component. Only those cases operated by the senior author were included in this series. We excluded all other operated cases to avoid surgeon′s bias and also to exclude learning curve period. Surgery was done in the patients with following clinical characteristics: (1) tumor well demarcated on gadolinium MR imaging; (2) relatively long clinical history (> six months); (3) clinically well-preserved-independent for all activities of daily living; and (4) tumor size < 2 cm was not strictly adhered to [5],[6] Patients were subjected to direct radiotherapy (without surgery) if the boundary of the tumor was ill-defined on magnetic resonance imaging (MRI), the tumor had a pure ventral location and/or patient had a rapid onset of clinical symptoms. These criteria have been based on the senior author′s experience over 25 years [Table - 1] and the same criteria also formed the basis of the proposed classification. (1) Expanding variety : Characteristics - (a) well-delineated lesion as seen on gadolinium contrast MRI located posteriorly, posterolaterally or ventrolaterally; (b) slow evolution of neurological deficits over a period of more than six months; (c) well preserved functional status, independent for all activities of daily living. (2) Infiltrating diffuse variety : Characteristics - (a) margins between the tumor and the surrounding parenchyma not well-differentiated, (b) short duration illness with rapid progression of neurological symptoms. (3) Ventrally located tumors : Characteristics - (a) ventral location of tumor without any lateral and posterolateral extension; (b) These tumors have been included in a different subset because of the ′very difficult to access′ surgical location. It has been felt by the authors to best leave these tumors alone as surgical intervention may cause more complications. According to the authors only the patients with ′ expanding variety ′ should be subjected for surgery. If surgery was undertaken, a radical removal was preferred. Radiotherapy was given only if the tumor was found to be malignant on histology. Patient population A total of 40 cases with ′expanding variety′ of brainstem glioma were operated over a 8.5-year period (January 1998-June 2007) personally by the senior surgeon (VSM). These patients were compared with 28 patients with ′ diffuse infiltrative ′ tumors and 4 patients with ′ pure ventral ′ tumors who were subjected to radiotherapy only (July 2003 - December 2006). Demographic and clinical profile Expanding variety Diffuse infiltrative and pure ventral variety The mean age was 5.2 years; (range 0.9-16 years). Of the 32 patients, 17 had symptoms onset less than three months, 12 had symptoms onset within six months and the remaing 2 had symptom onset between 6-12 months. The clinical features included pyramidal signs in 26 [hemiparesis in 16, quadriparesis in 19, 11 were dependent for all activities of daily living], and cerebellar signs in 16 cases. Investigations Z Contrast MRI was performed in all the patients. For the expanding variety , the tumor location was pons in 19, midbrain in 13, and medulla in 8. In d iffuse infiltrative variety, contrast MRI showed uniform enlargement of the brainstem axis without any differentiation between the tumor and the surrounding parenchyma [Figure - 1], while MRI in the ′ pure ventral ′ variety revealed ventral location of the tumor without any lateral extensions. Management Surgery was performed in all the 40 patients with ′ expanding variety ′ of brainstem gliomas. Surgery was performed in sitting (n = 20), prone (n = 10), lateral (n = 7), and supine (n = 3) positions. The sitting position was preferred for dorsal midbrain or upper pontine lesions. The prone position was preferred in dorsally situated lower pontine, medullary or cervicomedullary lesions. Lateral position was preferred in ventrolateral lesion of lower pons while supine position was used for ventrolateral midbrain or thalamic lesions. A midline suboccipital approach with or without vermian split was most commonly preferred (28) followed by retromastoid suboccipital cerebello-pontine angle approach (n = 7), subtemporal approach (n = 3) and supracerebellar infratentorial approach in two cases. Microsurgical techniques along with adjuvant instruments like the micro-CUSA (Valley Lab/ Sonoca), tissue vaporizer (Japan Medical Dynamic Marketing Inc), and intraoperative evoked potentials and brain mapping were used wherever indicated. In all the patients, a thin layer of brainstem parenchyma covered the surface. Cranial nuclei mapping was performed before incising the parenchyma over the floor of the fourth ventricle by the operating surgeon. This was performed in the following manner. Initially, the floor of the fourth ventricle was screened with bipolar electrodes using a 0.1-1mA single stimulus or at 10 Hz frequency runs at 50-400 ms. The responses were monitored using electromyography leads implanted within the orbicularis occuli, oris and the tongue. The lower cranial nerves were monitored by noting the hemodynamic/cardiac responses. The area with maximal response with least stimulus was identified to be the area closest to or at the cranial nerve nuclei. Incision over the parenchyma was always given over the thinnest part away from the nuclei if any. If there was decline of response during resection, the surgeon usually waited with saline irrigation before testing the response again and proceeding further with surgery. A radical resection (total or near total resection) was attempted in most patients . A thin layer of tumor tissue was left if it appeared not separable from the surrounding normal structure. All the patients were started on methylprednisolone just before making an incision on the brainstem and this was continued for 24-48 h. All patients were electively ventilated with sedation for 24-48 h. All cases of diffuse infiltrative (n=28) and pure ventral (n=4) brainstem gliomas (n=32 cases) were directly subjected to radiotherapy (fractionated with Co60). Results Expanding variety Histology revealed pilocytic astrocytomas in 10, Grade II in 17 and Grade III in 13. There was one death, due to aspiration. This patient had preoperative lower cranial palsy with the tumor location in the ponto-medullary axis and biopsy revealed a Grade III glioma. Postoperative MRI revealed a focal variety, however, at surgery it was found to be a diffuse variety with no clear-cut demarcation. One patient (one of the early cases) underwent a partial decompression. Following surgery, the patient had a poor respiratory reserve. There was deterioration of motor power after 24 h while on ventilator. Computed tomography (CT) scan showed swelling of the residual tumor with no hemorrhage. Patient was taken up for surgery and the tumor was decompressed radically. Patient improved following surgery, and she did require tracheostomy and tracheostomy care for four weeks. Complications included meningitis (two), wound infection (one), chest infection (five) and transient mutism (one). All these patients improved with appropriate treatment. Follow-up ranged from 3-68 months. Overall 35 patients improved or remained the same and three patients worsened in their clinical status at the time of discharge and one patient (as described above) after a transient deterioration improved. Follow-up MRIs performed in 28 patients revealed no residual tumors in 23 patients [Figure - 2] and [Figure - 3] and a very minimal residual tumor in five patients. All the patients with Grade I tumor are being followed up without radiotherapy while the patients with Grade II and III tumors were subjected to radiotherapy (either conventional Co or stereotactic radiotherapy). Sixteen patients, 14 with Grade I or II tumor, had a follow-up of more than two years. In one patient the ocular palsy improved during follow-up [Figure - 3]. Three patients with pilocytic astrocytomas had follow up for three, five and six years respectively without recurrence. Seven patients, four pilocytic astrocytomas; three, Grade II, had a follow- up ranging from 11-21 months. Of the 13 patients with Grade III gliomas, only three had a follow-up for up to two years following radiotherapy and chemotherapy. The maximal follow-up available for the other 17 patients was up to six months after which they were lost for follow-up. A Kaplan Meier curve is depicted showing the probability of survival for this group of patients [Figure - 4]. Diffuse infiltrative and pure ventral varieties Three patients were lost for follow-up after just one month following radiotherapy. Seventeen patients had a follow-up till three months, six till six months, four till nine months and only two had a follow-up greater than one year. It must be mentioned here that all these patients were treated on outpatient basis only. In India follow-up is generally difficult, particularly if the prognosis explained is grim and the patient′s attendants do not report deaths. There were four patients in the ′pure ventral′ group. In view of the location of the tumor these patients were deemed surgically inaccessible and were categorized under diffuse variety. They too received radiotherapy without a biopsy. Contrary to this group, surgical patients have a better follow-up as the patient and thier attendants are keen to have continued optimal treatment. Thus it would be difficult to comment on the actual survival of the patients based on these figures [Figure -4]. Discussion Various classifications of brainstem tumors have been proposed. [2],[3],[5],[6],[7],[9],[16],[17] Epstein [5],[6],[10],[17] and others [7],[8],[16],[18] have defined focal tumors as well-circumscribed masses with a diameter less than 2 cm. Any tumor larger than 2 cm is considered as diffuse tumor. We, however, included even tumors greater than 2 cm within the focal tumor category provided the lesion was well-defined and involved a focal area of the brainstem and the patient′s clinical features also suggested a focal pathology and relatively slowly progressive course. In addition we included only those patients with minimal neurological deficits and good functional life, able to attend all activities of daily living. In all the patients an attempt was made to perform excision as radically as possible. In instances where differentiation between the tumor and the surrounding normal parenchyma was difficult we left a thin rim of tumor. We have not taken tumor grading into consideration as some of our patients with Grade III tumor had clinical and MRI criteria to be included under well defined focal ′intrinsic′ lesion. We feel that the definition of ′diffuse′ should include only those tumors involving the brainstem axis homogenously with no differentiation between normal brainstem and the tumor. Based on our experience with these tumors, we propose a new classification [Table - 1]. We recommend surgery only for the ′ expanding variety ′ of tumors. This classification has some advantages: (1) It provides a simple surgical strategy whether or not to operate ′pure′ intrinsic tumors; (2) The classification does not emphasize on the 2 cm cut-off to differentiate between focal and diffuse tumors, This allows to consider surgery in some of the subset of tumors initially classified as ′diffuse′ if they fulfill other criteria of expanding variety of tumor; (3) This classification combines both biological and imaging characteristics. The surgery for focal ′intrinsic′ tumors remains one of the most challenging in neurosurgery. While radical excision is advised for these lesions, outcome is very much depends on the experience of the surgeon, completeness of tumor excision, and postoperative complications. Epstein [5] et al. , in their experience of treating 66 children with intrinsic brainstem tumors concluded that focal solid or cystic tumors are generally benign and should subjected to radical excision and this can result in a long-term survival. Qi-Wu Xu [8] et al. , have described 22 cases of solid brainstem tumors. Radical resection was performed in 20 patients, 19 were gliomas (astrocytomas or ependymomas). The study also included a few tumors with exophytic components. There were complications in 10 cases and one death. About 17 cases improved at the time of discharge. They concluded that tumors showing a focal solid nature on MRI should be subjected to a radical excision. Miyamoto et al. , [9] have recently described two patients with intrinsic midbrain pilocytic astrocytomas who had complete excision of the tumor and good long-term outcome without recurrence. Heffez et al. , [7] in their study have suggested the importance of a more aggressive approach in tumors, which appear focal and discrete on MRI. Apart from these studies, there have been few other reports [4],[19],[20] on the radical resection of truly intra-axial brainstem gliomas. Most of them have described focal ′intrinsic′ tumors as a part of their larger studies. In this series of highly selected 40 patients with expanding variety of brainstem tumor radical excision of the tumor was done by a single surgeon, which reduced the inter-surgeon bias. Overall, 35 patients improved or remained the same following surgery and three worsened. There was one death. One of the initial patient needed redo-surgery. Our experience suggests that these tumors need radical removal and is associated with good long-term outcome. Sixteen patients had more than two years follow-up. Two patients with pilocytic astrocytoma had follow-up for five and six years with no recurrence. One of the patient with ocular had complete improvement. We attempted to compare the expanding variety brainstem tumor group with 32 patients, 28 diffuse infiltrative variety, and four pure ventral, variety brainstem tumor group who were subjected to direct radiotherapy. The limitations for this comparison were, the analysis was retrospective and the time-frame of the two groups was different. In spite of these limitations, a few differences stand out prominently between the two groups: The mean age of the expanding variety group was much higher than the diffuse infiltrative variety and pure ventral variety group (19.2 vs. 5.2 years; P< 0.01). The duration of symptoms was much shorter in the diffuse infiltrative variety and pure ventral variety group and clinical progression much more rapid. Eighty per cent of patients with diffuse infiltrative variety and pure ventral variety group subjected to direct radiotherapy had much severe pyramidal symptoms than those compared with the expanding variety (67%). All these features suggest a more aggressive neurobiology for diffuse infiltrative and pure ventral varieties brainstem gliomas as compared with the expanding variety brainstem gliomas, These features may also corroborate the MRI morphology. Several authors have suggested that partial resection or biopsy combined with postoperative radiation is effective in many cases of focal, tumors, particularl, pilocytic astrocytomas. [4],[21] However, recurrence up to 20% has been reported in the literature with this approach. [21] Furthermore, malignant transformation has been reported as a significant sequel after partial resection. [22],[23],[24] The other limitation with this approach will be not including the malignant part of the tumor in the resection [25] One of our earlier patients deteriorated following partial removal possibly due to swelling of the residual tumor. While partial decompression may not cause such deterioration in exophytic tumors as these tumors have space to ′swell′ outside the brainstem axis. The identification of various subgroups of brainstem tumors has led to more rational treatment strategies and allows for a more accurate assessment of prognosis. The ′intrinsic′ tumors with paucity of neurological signs are a distinct subgroup of brainstem tumors (expanding variety). Most of them are low-grade astrocytomas and are amenable to radical surgical resection but this should be performed by an experienced surgeon in a setup with adequate intraoperative and postoperative facilities. Surgical intervention in this subgroup of brainstem tumors is associated with an excellent long-term prognosis. This is in contrast to the diffuse infiltrative and pure ventral group which should be subjected to radiotherapy only.[33] References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09082t1.jpg] [ni09082f2.jpg] [ni09082f3.jpg] [ni09082f1.jpg] [ni09082f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}