 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
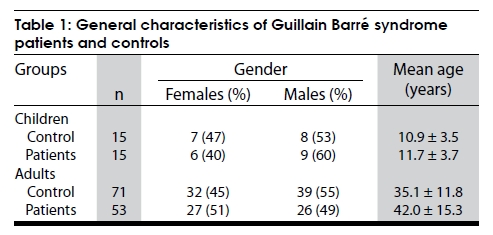
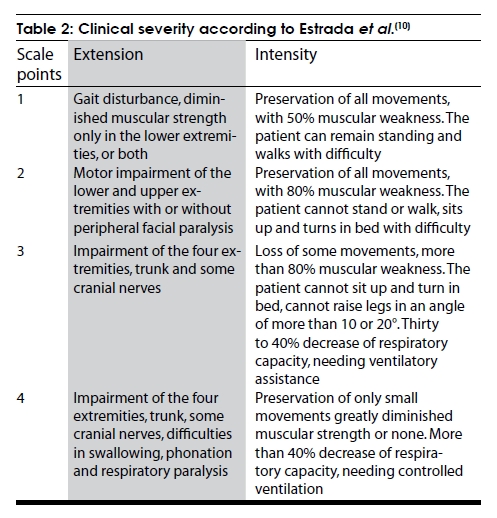
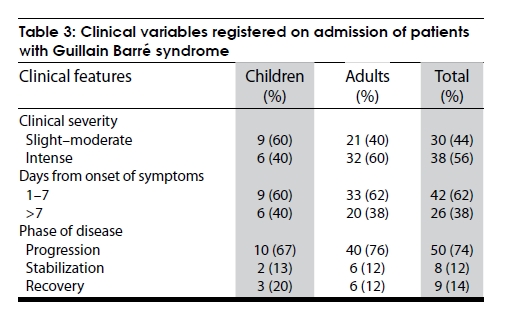
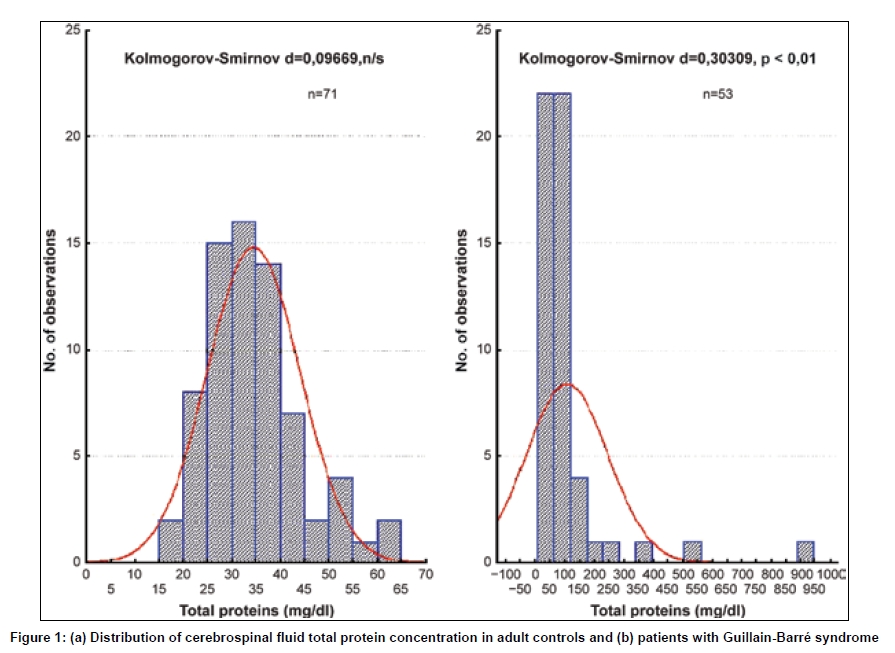
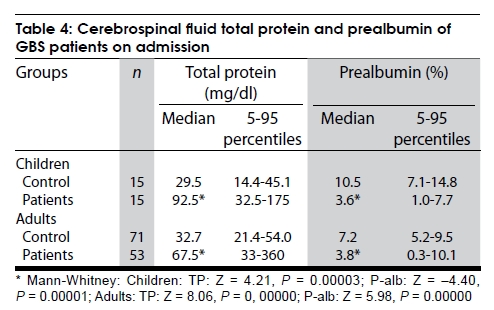
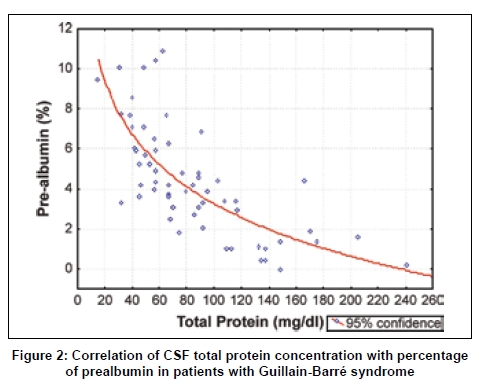
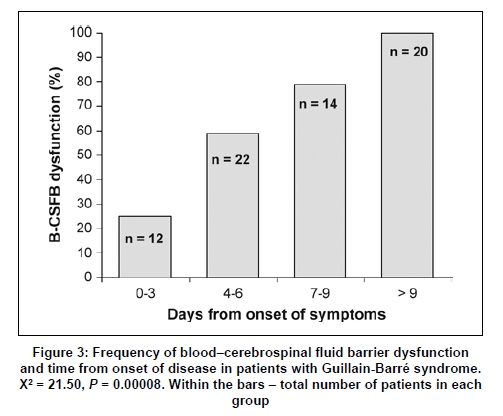
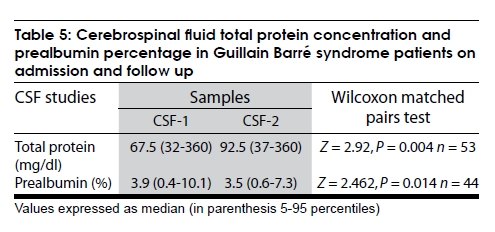
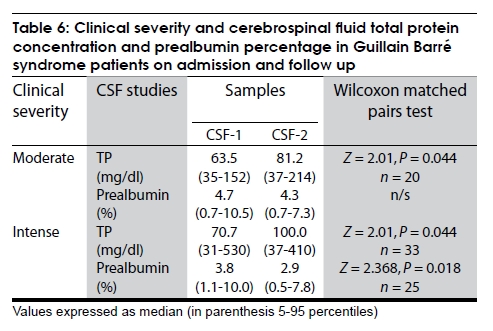
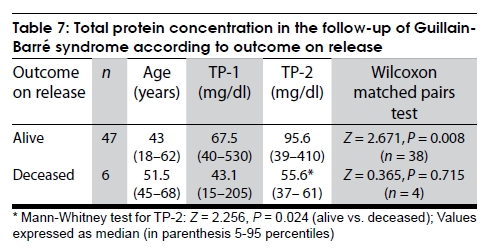
Neurology India, Vol. 57, No. 3, May-June, 2009, pp. 288-294 Original Article An appraisal of blood-cerebrospinal fluid barrier dysfunction during the course of Guillain Barré syndrome A. González-Quevedo, R. Fernández Carriera, Z. Lestayo O´Farrill, I. Suárez Luis, R. Mustelier Bécquer, R. S. Luis González Department of Neurobiology, Institute of Neurology and Neurosurgery, Havana, Cuba Correspondence Address: Dr. Alina González-Quevedo, Ave 299 # 22202, esq. 222. Reparto Fontanar, Boyeros. La Habana, Cuba aglez@infomed.sld.cu Date of Acceptance: 26-Feb-2009 Code Number: ni09085 PMID: 19587469 DOI: 10.4103/0028-3886.53282 Abstract Background: Elevated cerebrospinal fluid (CSF) total protein (TP) concentration (mainly due to a dysfunctional blood-CSF barrier (B-CSFB)) with normal cell count is a hallmark for the diagnosis of Guillain Barré syndrome (GBS). Aims: This work presents the evaluation of B-CSFB dysfunction with respect to the course, severity, and clinical features of GBS. Materials and Methods: A sample of CSF was collected on admission from 68 patients of both genders (15 children and 53 adults) diagnosed with GBS. A follow-up CSF sample was obtained approximately 15 days after admission. TP concentration was determined in the CSF and 7.5% polycrylamide gel electrophoresis was employed for serum and CSF protein fractioning. A low percentage of prealbumin fraction was considered a test of impaired B-CSFB. Results: Elevated TP concentration and lower prealbumin were observed in almost 70% of the patients on admission, but this percentage was lower (52.4%) during the first week from onset of symptoms. Both variables were directly associated with the time of evolution of the disease and also with a greater clinical severity. Follow-up CSF studies showed higher CSF TP and lower prealbumin percentages, while deceased patients did not display this response pattern in the follow-up CSF. Conclusions: B-CSFB dysfunction was present in only half of the patients with GBS during the first week from onset and it was directly associated with progression and clinical severity; nevertheless, a low B-CSFB dysfunction response during follow-up was associated with a lethal outcome, suggesting it could also serve a 'protective' effect during regeneration.Keywords: Blood-brain barrier, cerebrospinal fluid, Guillain Barré syndrome Introduction Guillain Barré syndrome (GBS) is an immune-mediated acute demyelinating disease of the peripheral nerves and spinal roots, and the most common type of rapidly evolving, generalized peripheral nervous system disorder. The diagnosis is usually established on the basis of symptoms and signs, aided by laboratory cerebrospinal fluid (CSF) findings and electrophysiological criteria. [1],[2] CSF analysis is mandatory as a diagnostic aid in the evaluation of inflammatory conditions involving the brain, spinal cord, and meninges. Elevated total protein (TP) concentration with normal CSF cell count (albuminocytologic dissociation) is a hallmark in acute and chronic inflammatory demyelinating polyneuropathies. [1],[2],[3] Protein levels may be normal during the first week of the illness, but the majority will have an increase in protein if measured two or three weeks later. [4] Elevated CSF protein concentration in GBS has been mainly associated with increased permeability of the blood-CSF barrier (B-CSFB). [5] The early invasion of the peripheral nervous system (PNS) by leukocytes is crucial to the pathogenesis of inflammatory demyelination. Circulating autoreactive T cells cross the blood-nerve barrier (BNB) and incite local inflammatory response. The breakdown of this barrier is one of the earliest morphologically demonstrable events in experimental allergic neuritis (EAN), [6] together with an increase in the concentration of immunoglobulin in the spinal roots, and reactive immune cell infiltration, [7] all related with the onset of neurological deficit. Abnormal gadolinium enhancement of intrathecal nerve roots in GBS seen on MRI images support the breakdown of the BNB. [8] The purpose of this study was to evaluate the status of the B-CSFB during the course of GBS, its association with the main clinical features, and its possible pathophysiologic implication in the different clinical phases. Materials and Methods Controls and patients Sixty eight patients (children and adults) who were admitted during four consecutive years at the Institute of Neurology and Neurosurgery of Havana with the diagnosis of GBS and eighty six controls were included in this study. The main demographic features of patient and control groups are shown in [Table - 1]. GBS was diagnosed taking into account the criteria established by the National Institute of Neurological and Communicative Disorders and Stroke (NINCDS) criteria for GBS. [9] The adult control group was comprised of patients undergoing surgery with spinal anesthesia with no known neurological disease. The control group for children consisted of subjects from 3-15 years of age, who underwent spinal puncture because meningitis was suspected, but was later discarded. The following data were registered on admission for each patient: Clinical severity, days from onset of disease, phase of disease (progression, stabilization, or recovery). Clinical severity was evaluated according to the scale proposed by Estrada et al. , [10] which measures extension and intensity of disease as shown in [Table - 2]. The final severity score was determined summing up the grades of extension and intensity and dividing them by two. Severity 1-2 in this scale was considered slight to moderate, while severity 3-4 was considered intense. Procedures for cerebrospinal fluid and serum sampling In all patients and child controls, 2 ml CSF were obtained on admission to the hospital as part of the diagnostic procedures, by nontraumatic lumbar puncture. In adult controls the CSF was taken previous to the administration of spinal anesthesia. Five milliliters of blood were extracted by venipuncture and collected in a dry test tube within two hours of CSF sampling. Blood and CSF were centrifuged within the first hour and the supernatants were stored at -20° C until analysis. A second CSF sample was withdrawn from 53 patients, 10-15 days after admission, following the same procedure described above. Analytical procedures Before centrifuging the CSF, total white cell count was carried out. CSF protein concentration (mg/dl) was determined in the supernatant employing Lowry´s spectrophotometric method [11] and expressed in mg/dl. Separation of CSF proteins was carried out by 7.5% polyacrylamide gel disk electrophoresis (PAGE) according to Ornstein and Davis′ method described in Smith, [12] followed by Coomassie R-250 staining. Gels were scanned in a DESAGA densitometer and the percentages of the protein fractions were calculated as described previously. [13] The percentage of prealbumin fraction (transthyretin) was registered, as it is considered indicative of impaired B-CSFB. Transthyretin in CSF originates predominantly from the choroid plexus, and when the B-CSFB is leaky, its percentage with respect to the rest of the CSF proteins, diminishes due to contamination with plasma proteins. [14] Taking into account the criteria established by Takeoka et al ., [15] the electrophoretic patterns of the stained gels were visually inspected to determine the B-CSFB permeability status. In order to measure the amount of change in TP concentration between the first and second CSF sample, the ratio TP1/TP2 was calculated for all patients. Statistical analysis Data analysis was carried out for the following variables: Age, gender, days from onset of disease, clinical severity, clinical phase of disease, outcome on release (survival or death), CSF TP concentration, prealbumin percentage, and dysfunction of B-CSFB. Data management and statistical analysis were conducted using Statistica 6.0 for Windows (Statsoft Inc, 2000). The frequency or percentage for the nominal variables was calculated. Chi-squared tests were used when comparing dichotomous variables. As TP concentration and prealbumin percentage were not normally distributed in patients, data are presented as median and 5-95 percentiles. The probability of a difference between two groups was assessed with the Mann-Whitney nonparametric U test, and Spearman rank correlations to study associations between quantitative variables. Wilcoxon matched pairs test was employed to compare two dependant variables (TP concentration and prealbumin percentage in CSF samples on admission and follow up). Statistical significance was declared for P < 0.05. Neurological, laboratory, and statistical assessments were performed separately without awareness of overall results. Results The main clinical features of the patients admitted with the diagnosis of GBS are shown in [Table - 3]. They were basically similar in children and adults, although clinical severity was somewhat higher in the latter. Most patients (74%) arrived in the progression phase of the disease, however, some were received when symptoms were stabilized or in recovery. All patients with less than one week from onset of symptoms on admission were in progression. Precedent events were not encountered in 19 patients (28%), while 49 patients referred some kind of event in the previous one to two weeks: Respiratory (21%), diarrheas (12%), dengue fever (15%), unspecific fever (6%), and others (18%). No association was found between the type of precedent event and the clinical and laboratory variables analyzed. Children and adults behaved similarly in this respect. Laboratory findings CSF analysis on admission showed normal cell counts (< 10 cells/mm 2 ) in all patients. The distribution of CSF TP concentration in adult controls and patients is shown in [Figure - 1]. In controls, TP concentration had a normal distribution, while this was not so in GBS patients. As CSF protein concentrations differ in children and adults, they were separated to calculate the median and 5-95 percentiles as shown in [Table - 4]. Both children and adult GBS patients had significantly elevated protein levels in the CSF on admission as compared to controls, although it should be noted that children tripled the control median value, while adult patients only doubled it. Coincidently, the percentage of the prealbumin fraction was diminished in both groups of patients with respect to their controls, more so in children. B-CSFB dysfunction, as evaluated by PAGE, was present in 69.1% of the patients on admission, but it was less frequent (52.4%) in patients studied during the first week after onset of symptoms. Spearman rank order correlation showed that CSF TP concentration was correlated with the duration of disease on admission ( r = 0.562, P < 0.001), while prealbumin percentage was inversely correlated ( r = -0.401, P < 0.01). This divergent behavior would be expected, considering TP concentration was inversely related to percentage of prealbumin in controls ( r = -0.431, P < 0.001) and patients ( r = -0.762, P < 0.0001) [Figure - 2]. The previous findings were concurrent with a higher frequency of B-CSFB dysfunction, when patients had more days of evolution of the disease [Figure - 3]. It should be noted that all patients who were studied with more than nine days after the onset of symptoms, displayed B-CSFB dysfunction. On the whole, severity of disease on admission was not associated with TP concentration, prealbumin percentage, or B-CSFB dysfunction. Nevertheless, when only those patients admitted during the first week from onset were included, TP was higher in patients with intense clinical severity (median: 68.1 mg/dl) than in those with moderate severity (median: 47.1 mg/dl) ( Z = 2.268, P = 0.023), and B-CSFB dysfunction was found to be more frequent in those where clinical severity was greater (65 vs. 29%, respectively) (c2 = 4.773, P = 0.03). Prealbumin percentage was not associated with clinical severity on admission, independently of the time of evolution (days from onset of symptoms). Follow-up cerebrospinal fluid studies Analysis of CSF protein studies during the follow- up of patients with GBS showed an increase of TP concentration and a decrease of prealbumin percentage in the second sample (CSF-2) with respect to the one taken on admission (CSF-1) [Table - 5]. Higher TP concentration in the second CSF sample was observed in patients with moderate and intense clinical severities, but prealbumin percentage was only lower in more severely affected patients [Table - 6] B-CSFB permeability was compromised in 52.4% of patients during the first week from onset of symptoms, while barrier dysfunction was significantly more frequent (83%) when the second CSF sample was analyzed (difference between proportions: P = 0.002). Oligoclonal bands in PAGE were observed in only one patient (1.5%). This patient recovered and was released without complications; nevertheless, eight years later he was admitted again with a similar neurological picture and died. Deceased patients Six adults and no children died during the course of disease (11.3% of all adult patients and 8.8% of the cohort of GBS patients). All deceased patients were above 45 years of age [Table - 7], they had significantly fewer days from onset of disease on admission than those who were released alive (medians: 4 vs. 7 days, respectively; Z = -2.002, P = 0.045) and had a higher score of clinical severity (medians: 4 vs. 2.5, respectively; Z = -2.602, P = 0.01). TP concentration on admission (TP-1) did not differ between these two groups; however, although only four of the deceased patients had a second CSF sample, TP-2 levels were significantly lower than in patients who were released alive ( P < 0.05). It should be noted that patients who were released alive displayed a significant increase in TP concentration in the second CSF sample, while deceased patients did not show the same behavior [Table - 7]. Discussion The present investigation in a cohort of GBS patients shows a similar pattern with respect to demographic characteristics and clinical presentation as described in the literature. [1],[2],[3],[16] The classical albumin-cytological dissociation described in GBS [3],[16],[17] was present in the majority of the patients studied at some moment in the course of the disease. We found that in our patients a PAGE pattern of B-CSFB dysfunction was present in almost 70% on admission. Nevertheless, almost half the patients admitted during the first week had normal CSF proteins and electrophoretic patterns, especially if clinical severity was not intense. It has been reported that CSF proteins can be normal during the first week of the illness. [3],[5] Hence timing of the measurement is critical. Isolated B-CSFB dysfunction is a frequent finding in CSF analysis, occurring in various neurological disorders, but most characteristically in GBS and chronic inflammatory demyelinating polyneuropathy (CIDP). [18] This study showed an increase of CSF TP concentration and a higher frequency of B-CSFB dysfunction during the follow-up of the illness, a feature corresponding with the association found between these variables and the days from onset of disease on admission. During the first week from onset, higher TP concentration and B-CSFB dysfunction were associated with a greater clinical severity. This could be a consequence of a greater swelling in the region of the spinal roots, affecting CSF reabsorption through arachnoid villi into the veins present in this region with subsequent reduction of flow and accumulation of proteins [19],[20] and/or intense inflammation at the junction of the dorsal and ventral roots causing a breakdown in the blood-nerve (spinal root) barrier and the transudation of plasma proteins into the CSF. [5] Sustained impairment of BNB has been related with worsening of GBS at the acute stage, as it allows continuous access of autoantibodies and proinflammatory cytokines from the systemic circulation to the PNS. [21] Our results also point to a greater impairment of the B-CSFB in more severely affected patients. Inflammatory cell transmigration from blood to nerve or spinal roots involves destruction of the basal membrane surrounding endoneural capillaries, a process where metalloproteinases (MMPs) are key participants and higher levels of circulating MMP-9 during progression of GBS have also been reported to correlate positively with disease severity. [22],[23] Several CSF protein components have been put forward as early diagnostic and prognostic biomarkers of PNS inflammation, [24],[25] but so far no reliable disease-related markers are available. Decreased prealbumin (transthyretin) in PAGE was related with B-CSFB dysfunction in our study. Proteomic analysis of the CSF has shown downregulation of transthyretin in GBS patients, although this seems to be an unspecific change in different inflammatory neurological diseases, [26],[27] most probably associated with barrier dysfunction. Signs of intrathecal synthesis of IgG have been reported in GBS patients with variable frequency, but it is mostly accepted that high CSF IgG concentration depends mainly on the degree of B-CSFB dysfunction, thus excluding the intrathecal origin. [5],[20],[28] In our series of GBS patients CSF oligoclonal bands were only observed in one patient, who completely recovered when this study was conducted, but died some years later when admitted with a very similar clinical picture. Considering that recurrence of GBS is not frequent, this is a feature worth investigating, due to its relevance as a possible prognostic factor. Wanschitz et al., reported a disease-specific enhanced intrathecal synthesis of αB-crystallin (αBC)-IgG antibodies in GBS, deeming that immune responses against αBC interfere with its anti-inflammatory and antiapoptotic properties, thus exacerbating the demyelinating process.[25] The death rate reported for GBS varies among different series, ranging from 5-13%, and occurring more often in the older age group. [29] In our cohort similar results were observed, but the most interesting finding was a lower response with respect to TP increase (an indirect quantitative expression of B-SCFB dysfunction) in the follow-up CSF samples of deceased patients, even though clinical severity was greater in these. A point worth noting in this study is that CSF TP concentration in the follow-up samples of children tripled their control values and none of them died, whereas adult patients only doubled their control values, while six of them died. Although the number of deceased patients was small, and this issue would warrant further investigation, the possibility that the damaged B-CSFB could be not only an inflammatory reaction of the spinal roots, but could also have a ′protective′ effect must be appraised, and some considerations can be made in this respect. Supporting this hypothesis are the findings in EAN indicating that MMPs in the inflamed PNS appear not only to promote inflammation but may also exert beneficial effects during regeneration of the damaged nervous system. [30] The pathological hallmark of the demyelinating autoimmune neuropathies is not only a macrophage-mediated demyelination, but macrophages also contribute to the termination of inflammation by promoting T-cell apoptosis and expressing anti-inflammatory cytokines including TGF-b1 and IL-10. [31] Intense B-CSFB impairment during the course of the illness is obviously not good, but the lack of response or a low response may have a negative prognostic effect. Thus, B-CSFB dysfunction in GBS could serve an important role after the acute inflammatory reaction subsides, to allow the passage of immune cells and substances to the nerve and spinal root during the regenerative process. In conclusion, the present study showed that increased CSF TP and B-CSFB dysfunction in GBS were more frequent with disease progression and were related to clinical severity; nevertheless, a low B-CSFB dysfunction response during follow-up of disease was associated with a lethal outcome, suggesting it could also serve a ′protective′ effect during regeneration.[Table - 3], [Table - 4] References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09085f2.jpg] [ni09085t3.jpg] [ni09085t6.jpg] [ni09085t4.jpg] [ni09085f3.jpg] [ni09085t5.jpg] [ni09085t1.jpg] [ni09085t2.jpg] [ni09085t7.jpg] [ni09085f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}