 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 3, May-June, 2009, pp. 300-303 Original Article The efficacy and safety of gabapentin in carpal tunnel patients: Open label trial A. Kemal Erdemoglu Ayhan Varlibas, Kirikkale University, Faculty of Medicine, Department of Neurology, Kirikkale, 07100, Turkey
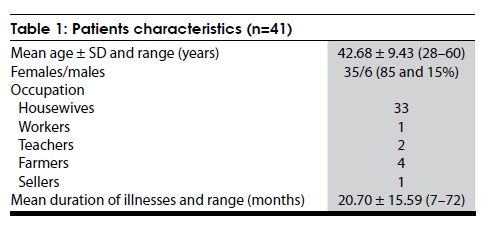
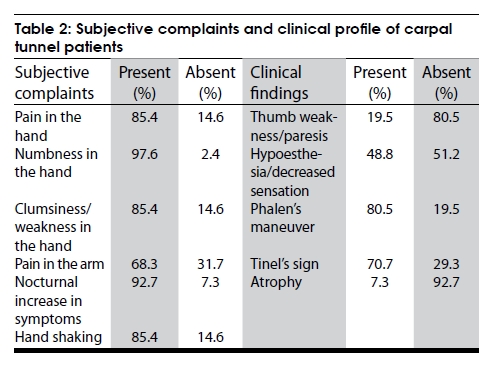
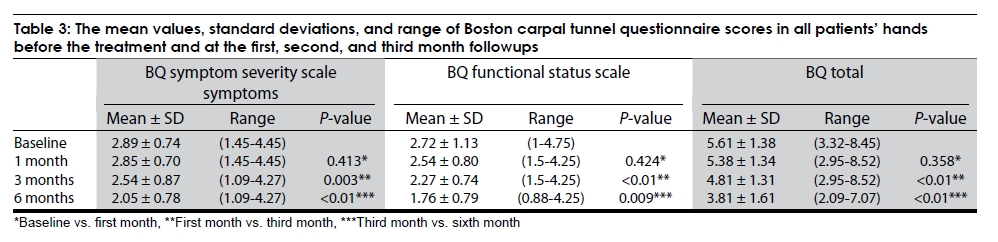
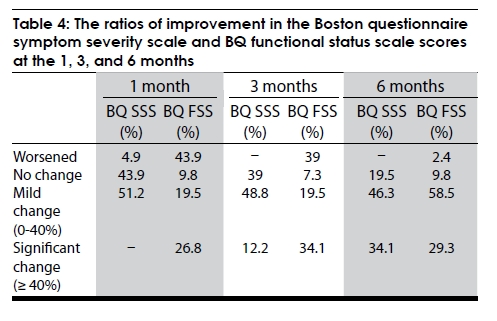
Correspondence Address: Dr. A. Kemal Erdemoglu, Kirikkale University, Faculty of Medicine, Department of Neurology, Kirikkale, 07100, TURKEY. Date of Acceptance: 12-Mar-2009 Code Number: ni09087 PMID: 19587471 DOI: 10.4103/0028-3886.53287 Abstract Background: Carpal tunnel syndrome (CTS) is the most common entrapment neuropathy caused by median nerve compression at the wrist. It results in loss of considerable man days and the effectiveness the various treatment modalities are still debated. Aim: To study the efficacy of gabapentin in patients with CTS. The study aim is to investigate the efficacy of gabapentin in patients with CTS patients who were refractory to the other conservative measures or unwilling for the surgical procedure. Materials and Methods: Forty one patients diagnosed as idiopathic CTS were included in the study. Patients were assessed with symptom severity scale (SSS) and functional status scale (FSS) scores of Boston Carpal Tunnel Questionnaire (BCTQ) before and at 1, 3, and 6 months of the treatment. Response to therapy was determined by using SSS and FSS scores of BCTQ. Results: The median dosage of gabapentin was 1800 mg/daily. Side effects were mild and transient. There was a statistically significant difference in both symptom SSS and FSS scores between before and after treatment in patient groups at the end of six months (P < 0.001). According to grading the changes in subscales of BCTQ, of 41 patients, 34.1 and 29.3 had a ≥ 40% decrease in SSS and FSS, respectively. Conclusion: Gabapentin was found to be partially effective and safe in symptomatic treatment of CTS patients.Keywords: Carpal tunnel syndrome, gabapentin, boston carpal tunnel questionnaire Introduction Carpal tunnel syndrome (CTS) is the most common type of entrapment neuropathy caused by median nerve compression at the wrist. It results in significant functional disabilities. Conservative treatment is often preferred treatment of choice. The effectiveness of other treatment modalities, topical injections and surgery, is still debated. [1] Conservative treatment includes: Splints, nonsteroidal anti-inflammatory drugs (NSAIDs), physical therapy, and ergonomic modifications. However the efficacy of these treatments is limited and recurrence of symptoms is common. [1],[2],[3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13] Surgery is indicated only when signs and symptoms of CTS are persistent and interfere with the quality of life.[14],[15] Surgery may not be acceptable for many patients. Gabapentin, an antiepileptic drug (ADE), is prescribed in various types of neuropathic pain conditions such as diabetic neuropathy, postherpetic neuralgia, plexopathies, and radiculopathies. [16],[17],[18],[19] This study evaluates the efficacy of gabapentin in the symptom alleviation in patients with CTS. Materials and Methods We studied 41 consecutive patients with CTS (37 women and 4 men, mean age 42.68 ± 9.43 years, range, 28 - 60 years). Patients with isolated CTS were included in the study and patients with CTS in the setting of other neurological diseases were excluded. The protocol was approved by the local ethics committee of our institution, and the informed consent was obtained from all study participants. Clinical diagnosis of CTS was based on the American Academy of Neurology diagnostic criteria [2] Comprehensive medical and neurological evaluations were performed to exclude neuropathies of other etiologies. Electrophysiological diagnosis of CTS was based on the criteria proposed by the American Academy of Neurology. [2] Boston carpal tunnel questionnaire (BCTQ), a self-administered disease-specific outcome instrument, was used to assess the severity of symptoms and the functional status. [20] The BCTQ has two subscales evaluating the clinical symptoms (symptom severity scale, SSS) and functional handicap (functional status scale, FSS). Symptom severity scale evaluates symptoms like pain, numbness, weakness, paraesthesia, or clumsiness using 11 questions. Functional status scale evaluates difficulties with daily activities like writing, buttoning clothes, holding a book while reading, gripping a telephone handle, opening jars, household chores, carrying grocery bags, and bathing/ dressing using eight questions. All answers were summed and the mean scores were calculated. The BCTQ has been validated into Turkish in a preliminary study recently. [21] Treatment and dosage Patients were started on gabapentin 300 mg/day initially and were advised to attend the clinic at weekly interval for titrating the drug dose. The drug dosage was titrated to a maximum of 3600 mg/day according to the tolerance of patients. The possible side effects were also monitored to assess the safety of the drug. Patients were asked to report or visit the clinic if any adverse effects appeared during the study period. Patients with the following conditions were excluded from the prescription of the drug: (1) known contraindication to or prior use of any AEDs; (2) creatinin clearance < 30 mL min or elevated liver enzymes, (3) clinically significant cardiovascular, renal, or hepatic disease; (4) history of narcotic or alcohol abuse; and (5) previous CTS surgery. Patients were asked to visit the clinic at 1, 3, and 6 months after the initial evaluation and the initiation of the gabapentin treatment. At every visit, patients were clinically evaluated and were asked to complete BCTQ to evaluate the efficacy of the treatment. Statistical analysis In statistical analysis, student′s t test, paired t test were used to compare the variables. The level of statistical significance was P < 0.05. Results Patient characteristics Of the 47 evaluated patients, 6 patients were excluded by the exclusion criteria. There were 35 females, mean age was 42.7 years (range, 28-60) and mean duration of symptoms was 20.7 ± 15.59 months (range 7-72) [Table - 1]. Clinical findings The symptoms were right hand in 18, left hand in 16 and both the hands in 7. In 19 patients paresthesiae were present in the first three fingers and in 22 patients it was in all the fingers. Most of the patients had numbness, tingling (97.6%), and nocturnal worsening of symptoms (92.7%) as the initial presentation [Table - 2]. Almost 49% patients had numbness in the distribution of the median nerve. Phalen′s maneuver was positive in 80.5% patients and Tinel′s sign was positive in 70.7% patients. Boston carpal tunnel questionnaire findings The BCTQ subscale scores before the initiation of gabapentin and at the end of 1, 3, and 6 months are shown in [Table - 3] and [Table - 4]. There was a significant decline in the SSS scores at the end of third and six months of treatment [Table - 3] and [Table - 4]. Similarly the decline in the FSS scores was significant at the end of the study [Table - 3] and [Table - 4]. Dosage and compliance The median dose of gabapentin was 1800 (range: 900-3600 mg). Drug dosage was titrated up to 3600 mg unless there were side effects at such levels. All subjects who completed the first three months of study were considered to have a good compliance to the treatment. Side effects observed were: Gastrointestinal disturbance ( n : 8) and drowsiness ( n : 3). Gastrointestinal disturbance and drowsiness were the most common side effects in the first month of treatment. Although side effects were seen in 26.8% of patients, most of them were mild and tolerable. Discussion This study clearly shows the efficacy and safety of gabapentin in the symptomatic treatment of CTS. We used the most objective BCTQ symptom severity and functional interference subscores to evaluate the efficacy of the drug. There have been a number of clinical studies showing the efficacy of gabapentin in neuropathic pain such as trigeminal neuralgia and postherpetic neuralgias., [16],[17],[18],[19] Only two studies evaluated the efficacy of gabapentin in the symptomatic treatment of CTS.[22],[23] Duman et al . [22] reported an improvement in the symptoms in 21 patients with CTS patients treated for three months. The mean dosage of gabapentin was 648.00 ± 112.25 mg/d (range, 600-900 mg/d), a lower dosage than this study. Taverner et al . [23] found improvement and/or remission of symptoms in 84.2% of patients with CTS treated with gabapentin for six mont The recommended dose of gabapentin in patients with epilepsy is 900-3600 mg/ day. We initiated the patients with a dosage of 300 mg/ day and increased up to 3600 mg according to the patient′s tolerance and requirement. The side effects in our study were transient and mild. Antiepileptic drugs have been widely used in the treatment of neuropathic pain for the reason that the fundamental mechanisms being similar with some epilepsy and neuropathic pain models. However there is a limited understanding of the mechanism of action of these agents. Antiepileptic drugs depress abnormal neuronal discharges and raise the threshold for neural impulse propagation. Recent studies have shown the efficacy of new AEDs such as pregabalin, lamotrigine, and gabapentin in neuropathic pain. Gabapentin has been shown to provide significant analgesia in several neuropathic pain conditions, including trigeminal neuralgia and peripheral diabetic neuropathy, and may also be effective in treating neuropathic pain refractory to other antiepileptics. [16],[17],[18],[19] Gabapentin acts on modulating voltage-dependent calcium channels and glutamate uptake, the mechanism by which gabapentin relieves pain is under investigation. The major limitation of this study was not having a control arm. This would have allowed us to study the placebo effect on various parameters studied. However our study is the only study that has shown the longterm efficacy and safety of gabapentin in the symptomatic treatment of CTS. We feel that gabapentin can be the drug in patients with persistent symptoms who are reluctant to have surgery and also in patients with persistent symptoms following surgery. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09087t2.jpg] [ni09087t4.jpg] [ni09087t3.jpg] [ni09087t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}