 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 3, May-June, 2009, pp. 313-319 Brief Report Intra-arterial thrombolysis in basilar artery occlusions combination of intra-arterial thrombolytics and Gp IIb/IIIa inhibitors in basilar artery thrombosis S. B. Gaikwad, M. V. Padma1 , E. J. Moses, Kanika Sethi, M. Tripathi 1 , R. Bhatia1 , K. Prasad1 , N. K. Mishra Departments of Neuroradiology, 1 and Neurology, All India Institute of Medical Sciences, Ansari Nagar, New Delhi -110 029, India
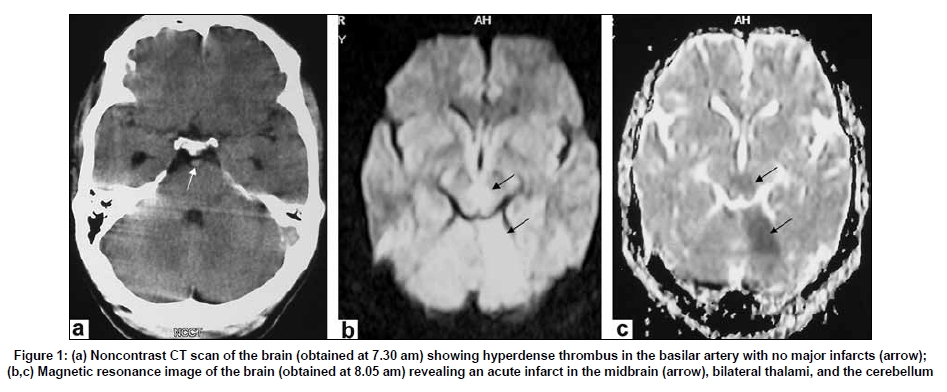
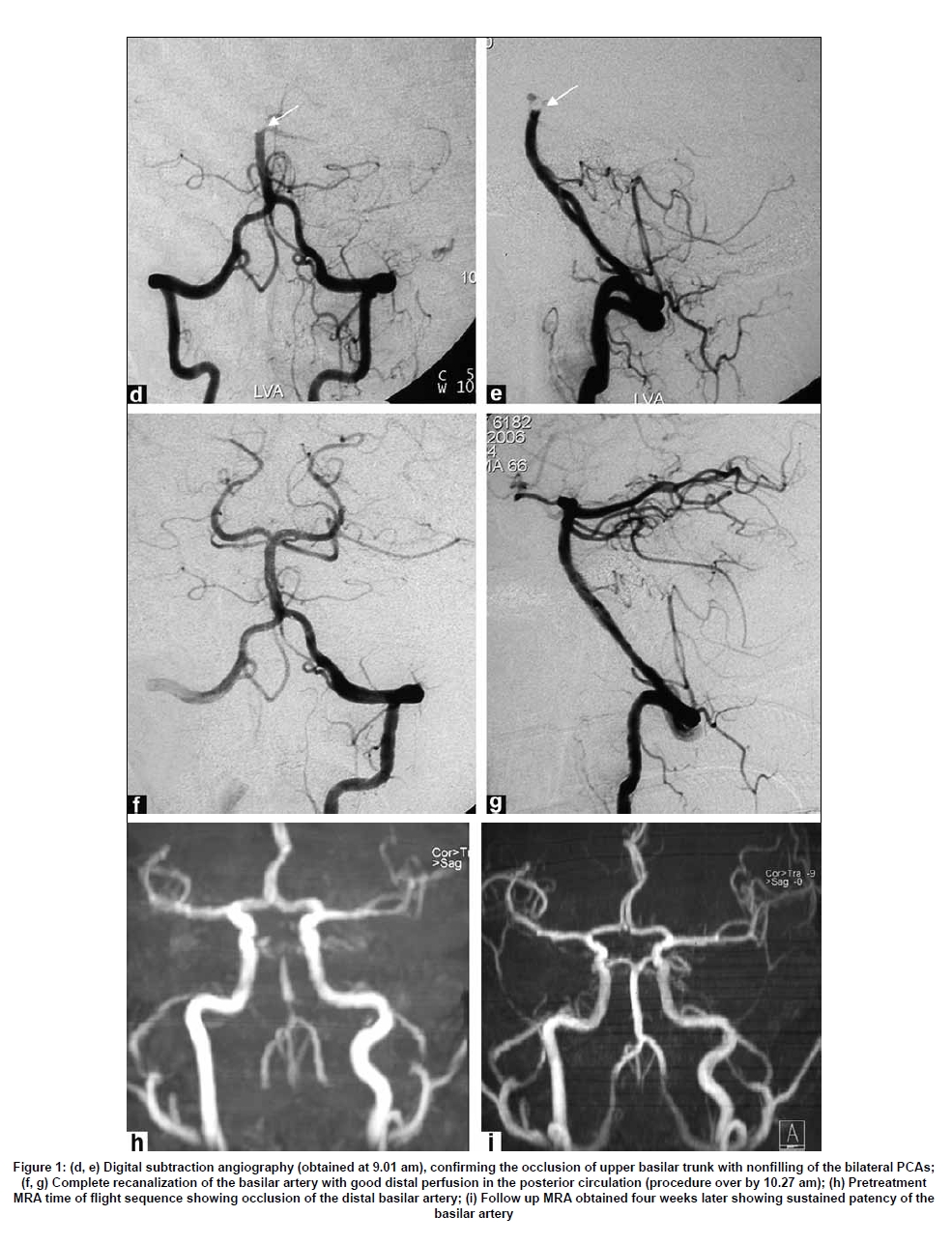
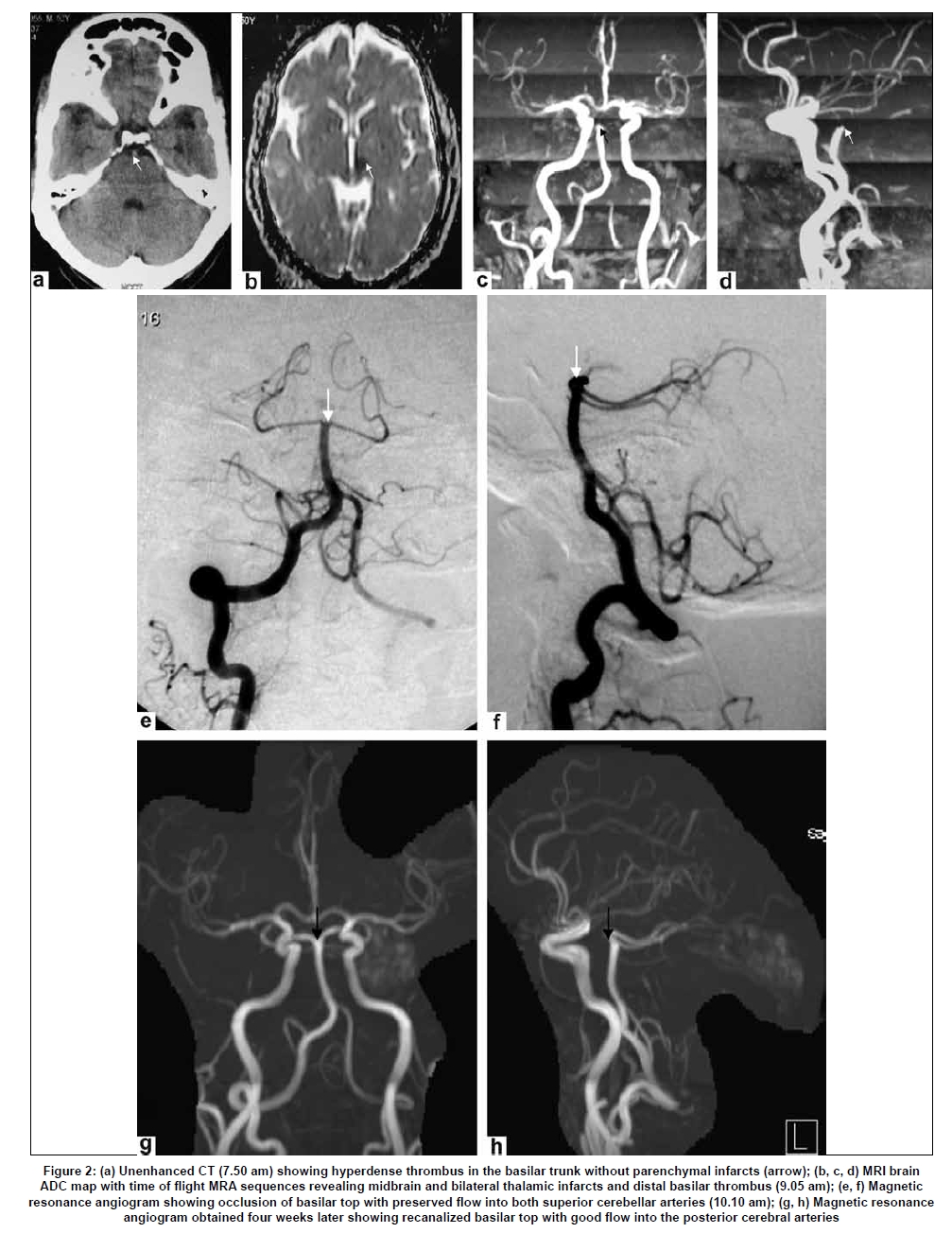
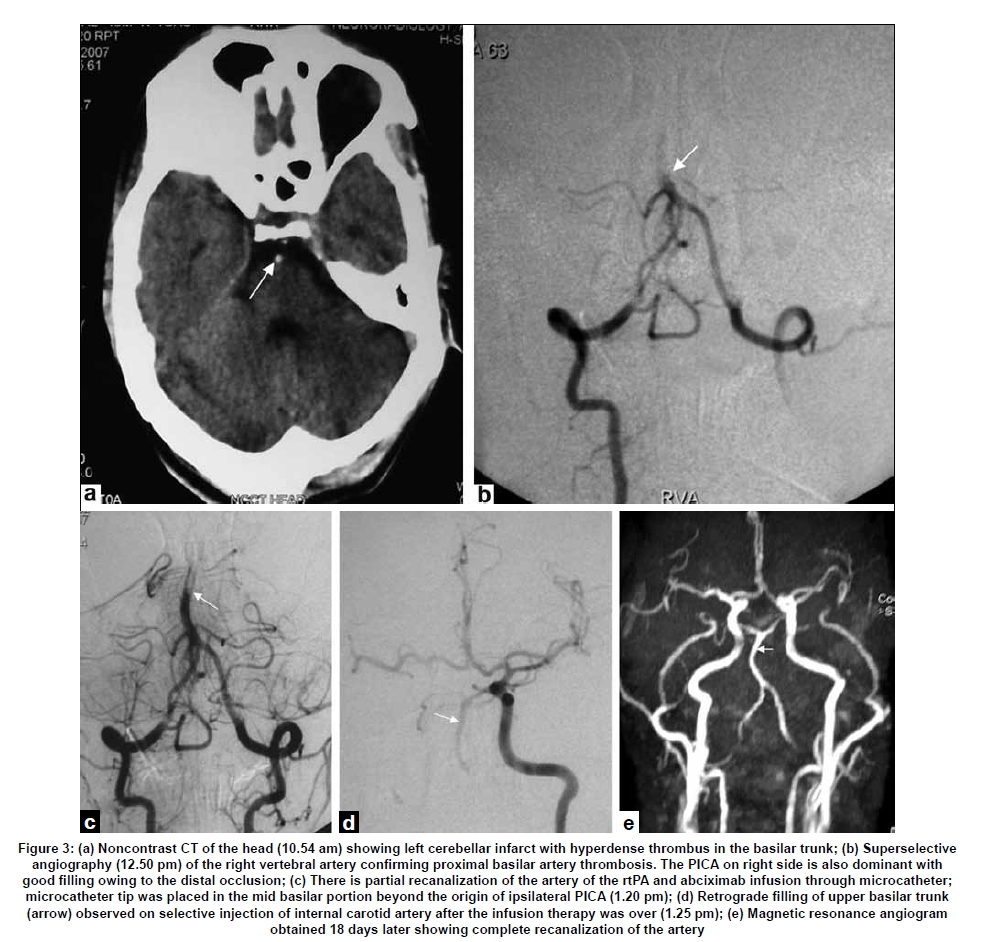
Correspondence Address: Dr. Shailesh B. Gaikwad, Department of Neuroradiology, All India Institute of Medical Sciences, Ansari Nagar, New Delhi -110 029, India. Date of Acceptance: 31-Mar-2009 Code Number: ni09091 PMID: 19587474 DOI: 10.4103/0028-3886.53291 Abstract Basilar artery thrombosis has high morbidity and mortality. Though intra-arterial thrombolytics have proven efficacy in the treatment of acute basilar artery occlusion, the elevation of procoagulant factors in the blood after intra-arterial thrombolysis could result in subsequent thrombus formation and clinical deterioration. Glycoprotein IIb/IIIa inhibitors have been shown to reduce this elevation in procoagulants. We present a pilot study of three cases of acute basilar artery occlusion treated with a combination of intra-arterial thrombolytics and Gp IIb/IIIa inhibitor with remarkable clinical recovery seen in all the patients.Keywords: Basilar artery thrombosis, glycoprotein IIb/IIIa inhibitor, intra-arterial thrombolysis Introduction Basilar artery thrombosis is a serious condition and commonly affects the elderly with male preponderance. If untreated it is usually fatal in most cases or severely disabling. [1] In acute basilar artery occlusion intra-arterial (IA) thrombolysis has been shown to be associated with good outcomes. [2],[3],[4] Recent studies in acute myocardial infarction have demonstrated that thrombolytic and glycoprotein IIb/IIIa receptor inhibitor agents have a synergistic effect in achieving rapid and complete arterial recanalization without associated increase in severe hemorrhagic complication.[5],[6],[7]. Only few studies have reported a combination of systemic (intravenous) recombinant tissue plasminogen activator (tPA) and tirofiban, a nonpeptide glycoprotein IIb/IIIa inhibitor, in acute basilar artery thrombolysis. [8] We describe our experience of treating three patients with acute basilar artery occlusion with a combination of tPA and abciximab given locally into the proximal thrombus interface intra-arterially. Case Reports Case 1 A 29-year-old male with no known risk factors presented with sudden onset vertigo, dizziness, hyperesthesia, rapid onset right hemiparesis, diplopia, and drowsiness. On neurological examination a admission, within three hours ollowing onset of stroke, he was in coma with bilateral complete ophthalmoplegia and right-side hemiplegia. Noncontrast computerized tomography (NCCT) scan of the brain [Figure - 1]a showed hyperdense thrombus in the basilar artery with no major infarcts. Magnetic resonance imaging (MRI) of the brain revealed an acute infarct in the midbrain, bilateral thalami, and the cerebellum with midbasilar artery occlusion [Figure - 1]b and c. Digital subtraction angiography (DSA), [Figure - 1]d and e confirmed the findings seen on MR-angiography (MRA). Local IA thrombolysis was initiated with tPA (mixed as 1 mg per milliliter saline) with small aliquots of 5 mg per injection into the proximal thrombus interface. After IA application of a total dose of 20 mg, the final superselective angiogram revealed partial recanalization of the basilar artery. This was then followed by IA infusion of aliquots of 2 mg each of abciximab till a dose 4 mg was reached. Following which, there was complete recanalization of the basilar artery with good distal perfusion in the posterior circulation [Figure - 1]f and g. Within six hours of thrombolysis, the patient started to improve. The follow-up CT scan revealed no hemorrhage. All investigations for cause of stroke were negative. At the time of discharge at one week he was alert with mild nondisabling incoordination in gait, bilateral mild ptosis, and left sixth nerve palsy. Follow up at three months showed only residual left sixth nerve palsy. A repeat cerebral MRA [Figure - 1]h (pretreatment), I (post-treatment)] four weeks later showed sustainable patency of the basilar artery. He has had more than two years of clinical follow up and except for partial sixth nerve palsy he is fully recovered. He is on aspirin 150 mg for secondary prevention. Case 2 A 52-year-old man, a known hypertensive, presented with sudden onset vertigo with sweating and immediate unconsciousness. Three years before this illness he had left hemiparesis from which he improved completely. On evaluation, within five hours of stroke in the Emergency Department (ED), he was in coma and his left pupil was dilated and nonreacting with bilateral pyramidal signs. Noncontrast computerized tomography of the brain was normal except for hyperdense thrombus in the basilar trunk [Figure - 2]a, arrow]. MRI brain with time-of- flight (TOF) MRA sequences revealed midbrain and bilateral thalamic infarcts and a distal basilar thrombus [Figure - 2]b-d. Superselective angiogram was performed and local (IA) infusion of 20 mg of tPA was given. Check angiogram revealed a partial recanalization of the basilar artery [Figure - 2]e and f. A total of 10 mg of abciximab was given locally in small doses of 2 mg each till a good antegrade flow was established. Subcutaneous low molecular weight heparin was given for a period of seven days following thrombolysis. Clinically, the patient improved remarkably within the next 48 hours. He became ambulant within a week of onset of stroke and was discharged on the fourteenth day with a modified Rankin score (mRS) of 2. A follow up MRI showed complete recanalization of the basilar artery with flow in both the posterior cerebral arteries [Figure - 2]g and h. Investigations showed moderate left ventricular dysfunction and hypokinetic apex. He was presumed to have a cardioembolic event and was discharged on oral anticoagulants with an advice to maintain an INR of 2-2.5. Case A 48-year-old man presented with history of sudden onset of altered sensorium of four hours duration prior to presentation into the ED. There were no seizures or headache at onset. He had no known vascular risk factors except chronic smoking. On examination, he was responsive feebly to painful stimuli, his right pupil was dilated with sluggish reaction to light, and there was a left facial palsy, right hemiplagia, and bilateral pyramidal signs. Noncontrast computerized tomography brain showed left cerebellar infarct with hyperdense thrombus in the basilar trunk [[Figure - 3]a, arrow]. Superselective angiography confirmed proximal basilar artery thrombosis and nonfilling of the entire basilar artery suggesting a long column of thrombus and a large thrombus burden [Figure - 3]b. Owing to the proximal occlusion in the basilar artery and also due to the preferential flow into the dominant right posterior inferior cerebellar artery (PICA), it gave an impression that right vertebral artery (VA) is ending in PICA [Figure - 3]b. Tissue plasminogen activator was infused (total dose of 20 mg) followed by 10 mg of abciximab with establishment of good antegrade flow up to the distal basilar artery [Figure - 3]c. Retrograde filling of upper basilar trunk was observed on selective injection of internal carotid artery [[Figure - 3]d, arrow]. Owing to the large thrombus burden, partial and significant recanalization could be achieved within the limited doses of the combined thrombolytics and antiplatelet. Since good collateral flow was noticed in the retrograde direction [[Figure - 3]d, arrow] with opacification of the upper basilar, we decided to stop at this moment to prevent from exceeding the dose limits to avoid hemorrhagic complications. Post thrombolysis, the patient′s sensorium improved over the next 24 hours. His hemiparesis also improved but remained ataxic. At the time of discharge he could walk with support but continued to have combined vertical and horizontal gaze palsy with left skew and vertical diplopia. The right pupil was still dilated and nonreactive to light. One month after discharge, the patient′s horizontal gaze palsy completely resolved. MRA obtained 18 days later showed complete recanalization of the artery [Figure - 3]e. A complete recanalization of the occluded artery on follow up MRA 18 days after the procedure proves the often stated point that tPA does have a continued and sustained action once it binds with the thrombus following its delivering into the thrombus through the microcatheter. The microcatheter tip was placed in the mid portion of the thrombus which enabled us to infuse the tPA in the midbasilar segment well beyond the origin of the right PICA. This also ensured effective and targeted delivery of the drug. Discussion Review of the literature found very few case studies reporting the combination therapy. [8] Junghans and colleagues were the first group to report the use of IA tPA with intravenous tirofiban for treating acute basilar artery thrombosis. They treated four patients with this combination and found rapid and sustained clinical improvement in all and also demonstrated patency of the intracranial vessels. [8] Intra-arterial thrombolysis has been shown to be as effective or superior to intravenous thrombolysis in lysing the clot as well as improving patient outcome. [9],[10] It has been documented that markers of procoagulant activity may increase tremendously immediate post-treatment with tPA (peaks after 1-3 hours and persists for up to 72 hours), indicating that thrombolysis may trigger the coagulation cascade and hence further enhance thrombin formation at the site of occlusion [11] . This may be one explanation for recanalization failures seen at times with tPA administration. The role of glycoprotein IIb/IIIa receptors and their role in the coagulation cascade have been well elucidated. [12] Activated glycoprotein IIb/IIIa receptor binds fibrinogen molecules, which form bridges between adjacent platelets thereby facilitating platelet aggregation and accumulation. Thrombin increases fibrin deposition favoring incorporation of platelets into the thrombus in the downstream vascular territories and may obscure heparin-binding sites impeding heparin to prevent reocclusion. Thus, glycoprotein IIb/IIIa inhibitors inhibit this aggregation of platelets which occurs secondary to a successful thrombolysis. Selective catheterization of the target vessel along with administration of thrombolytic agents into the thrombus is now considered most optimal for faster, more complete recanalization of the acute basilar occlusion. Complete reperfusion of the posterior circulation is taken as a conditional sine qua non for most favorable stroke outcome after basilar artery occlusion. Although IA thrombolysis has been proven optimal, this procedure requires expertise and adequate infrastructure which makes it amenable only to few selected centers. With this in view, some case series have also been reported using intravenous delivery of the fibrinolytic agent and glycoprotein IIb/IIIa receptor blocker as infusion over several hours. Alex Abou-Chebl et al. [13] have suggested a multimodal therapy for severe ischemic stroke combining GpIIb/IIIa antagonists and angioplasty after failure of thrombolysis. All the three patients treated within 6-8 hours of onset of stroke with combination of fibrinolysis and glycoprotein IIb/IIIa receptor blocker have done extremely well with outcome of mRS less than 2. No symptomatic or asymptomatic cerebral or extracerebral hemorrhagic complications were observed. None of the patients developed thrombocytopenia, known to occur with glycoprotein IIb/IIIa receptor inhibitor administration. It is well known that abciximab can cause thrombocytopenia if used in larger doses and for prolonged period. Knowing this fact fully, we decided to use small doses of IA infusion to maximize the drug effectiveness and offset its potential adverse effects. To have sustained antiplatelet action all our patients were put on aspirin 150 mg per day (life-long) and clopidogrel for the first three months. Regular blood tests were carried out to detect any suggestion of thrombocytopenia. Though our cohort was small, only three patients, we found that a combination of small doses (8-10 mg) of abciximab and tPA administered intra-arterially resulted in rapid and sustained recanalization of the basilar artery with rapid improvement in the clinical condition of the patient without significant hemorrhagic complication. We further wish to indicate that the combination of rtPA and antiplatelet is investigational at the moment and we do not wish to draw any meaningful conclusions from our small pilot study. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09091f1d-i.jpg] [ni09091f1a-c.jpg] [ni09091f3.jpg] [ni09091f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}