 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 3, May-June, 2009, pp. 324-326 Case Report Spontaneous intracranial extradural hematoma: Case report and literature review Fan Xue Zheng, You Chao Department of Neurosurgery, West China Hospital, Sichuan University, Chengdu Sichuan, 610041, P.R. China
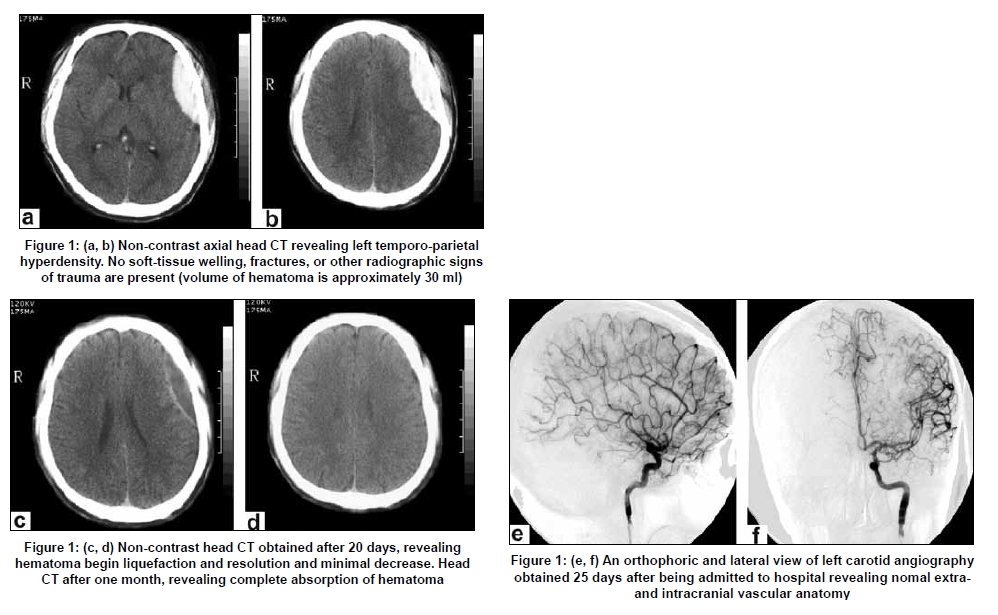
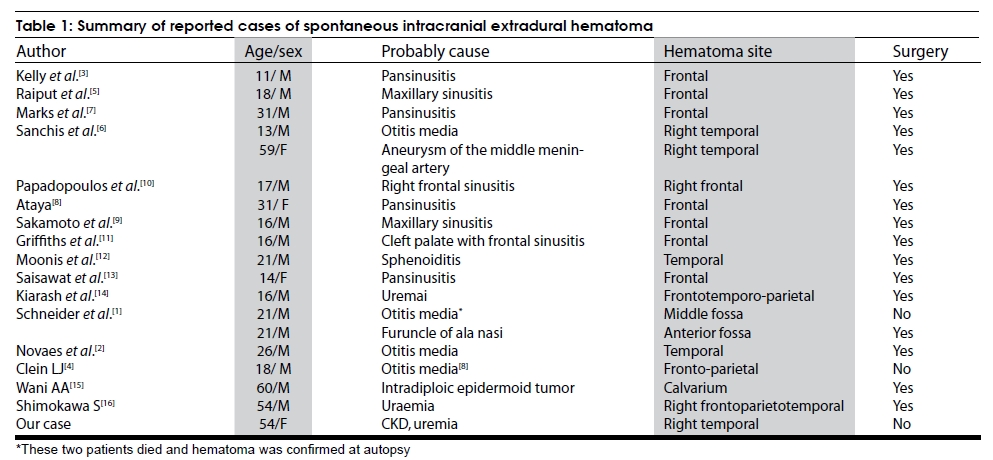
Correspondence Address: Dr. You Chao, Department of Neurosurgery, West China Hospital of Sichuan University, 37 Guo Xue Xiang, Wu Hou District, Chengdu - 610 041 China. Date of Acceptance: 24-Jan-2009 Code Number: ni09093 PMID: 19587476 DOI: 10.4103/0028-3886.53288 Abstract Spontaneous extradural hematoma (EDH) is an uncommon form of intracranial hematoma and is caused by the adjacent sinus and otic infections, dural vascular malformations and disorders of blood coagulation. We report spontaneous EDH in a 54-year old women with chronic kidney disease (CKD) on intermittent hemodialysis. She was successfully managed by conservative treatment. The EDH in her was probably related to the coagulation abnormalities associated with CKD, hemodialysis or heparin use during the dialysis.Keywords: Extradural, hematoma, intracranial, spontaneous Introduction Spontaneous extradural hematoma (EDH) is a very uncommon intracranial hematoma and is caused by adjacent infections, dural vascular malformations, tumors, disorders of blood coagulation. Till date there are 18 such documented cases in the literature. [1],[2],[3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14],[15],[16] The first documentation of spontaneous EDH was by Schneider and Hegarty in 1951. [1] We report spontaneous EDH in patient with chronic kidney disease (CKD) on intermittent hemodyalisis. Case Report A 54-year-old woman a known case of CKD (chronic glomerulonephritis) on intermittent haemodialysis between 2000 and 2007 was admitted for sudden onset headache associated with vomiting. Her medical history was otherwise unremarkable. There was no history any head trauma or trivial injury. On neurological examination she had mild clouding of consciousness and right side weakness (grade 3/5). Glasgow coma scale score was 12/15 (E3 V4 M5). Pupils were bilaterally reactive. Her vitals were normal. She was markedly anaemic, hemoglobin 7 g/dl. Coagulation profile was: Partial thromboplastin time 32.4 s (reference range 21.8-31.5 s), a prothrombin time of 1.20 (reference range 0.75-1.19), and platelet count 100,000/m 3 (reference range 130-400,000/mm 3 ). Blood urea nitrogen was 36 mg/dl (reference range 8-22 mg/dl) and serum creatinine 8.3 mg/dl (reference range 0.5-1.3 mg/ dl). An urgent non-contrast CT scan showed left-sided temporoparietal EDH [Figure - 1]a and b. A diagnosis of spontaneous EDH and CKD was made. The patient received a conservative management including mannitol and etamsylate. At the same time she also received transfusion of fresh frozen plasma 800 mL, cryopreciptitate 5.0 units, fibrinogen 3.0 grams and lyophilized prothombin complex concentrate (LPCC) 1400 units. A repeat CT done after 20 days showed resolving hematoma [Figure - 1]c Digital subtraction angiography (DSA) done after 25 days of the ictus to ascertain the reasons of hematoma was normal. [Figure - 1]e and f. A month later, she was asymptomatic and CT scan demonstrated complete resolution of haematoma [Figure - 1]d. During a 6-month follow-up, she remained well with no neurological deficit and she was being treated for CKD with intermittent haemodialysis. Discussion Spontaneous EDH is an uncommon neurological emergency and requires urgent investigation and treatment. Till date including our case only 19 cases [Table - 1] were documented in the literature. [1],[2],[3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14],[15],[16] Of the 18 patients documented in the literature, adjacent cranio-facial infections were the causes in 14 patients: Paranasal infection in nine (3, 5, 8-13), chronic otitis in four (1, 2, 4, 6), and furuncle on the ala nasi in one (1). The proposed mechanism was intracranial spread of the infection from the craniofacial site and the vasculitis associated with the infection, bleeding from the rupture of vasculitic vessel and subsequent expansion. [8],[9],[10],[11] In all these, except the patients who died, hematoma was evacuated by surgery and the patients were subsequently exposed to antibiotics. In one of the patients the EDH was due to rupture of the aneurysm of middle meningeal artery proven by pre-operative cerebral angiogram. The hematoma was surgically evaculated. [6] In the patient reported by Wani et al ., [16] there was erosion of the vessels by the intradiploic epidermoid tumor. Intracranial hemorrhages, intracerebral, [17] subdural, [18] and EDH [14],[16] have been documented in patients with CKD and uremia. However the exact mechanism for this complication is uncertain, the possible mechanisms may be more than one. In our patient underlying vascular malformation was excluded by cerebral angiogram Probably the coagulation abnormalities associated with uremia, heparin use during the hemodialysis or hemodialyis per se may be the factors for the EDH. In her both the partial thromboplastin time and prothrombin time were in the upper limit of normal and platelet count was on the lower limit of the normal. However we have not done the platelet function tests. Platelet dysfunction has been documented in patients with uremia. [19] In uremia nitric oxide may inhibit platelet activation, adhesion and aggregation by activating the platelet guanylate cyclase. [20] During hemodialysis there can be changes in the serum and cerebrospinal fluid osmolality which can result in intracranial pressure fluctuations. [21] It is possible that such changes may cause vascular damage and bleeding. In uremic patients with spontaneous EDH surgery can be avoided as the mechanism of bleeding is multifactorial and the coagulation abnormality should be corrected. However surgery may be indicated if the patient has midline shifts, elevated intracranial pressure, and progressive clinical deterioration. We managed our patient conservatively as she had no evidence of midline shifts. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09093t1.jpg] [ni09093f1.jpg] |
| |||||||||

{kind=link}
{kind=link}