 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 3, May-June, 2009, pp. 357-358 Letter To Editor Rapid resolution of hydrocephalus due to simultaneous movements of hematoma in the trigono-occipital horn and the aqueduct Naoshi Hagihara, Toshi Abe1 , Kohei Inoue, Mitsuo Watanabe, Kazuo Tabuchi Department of Neurosurgery, Koyanagi Memorial Hospital, Saga.
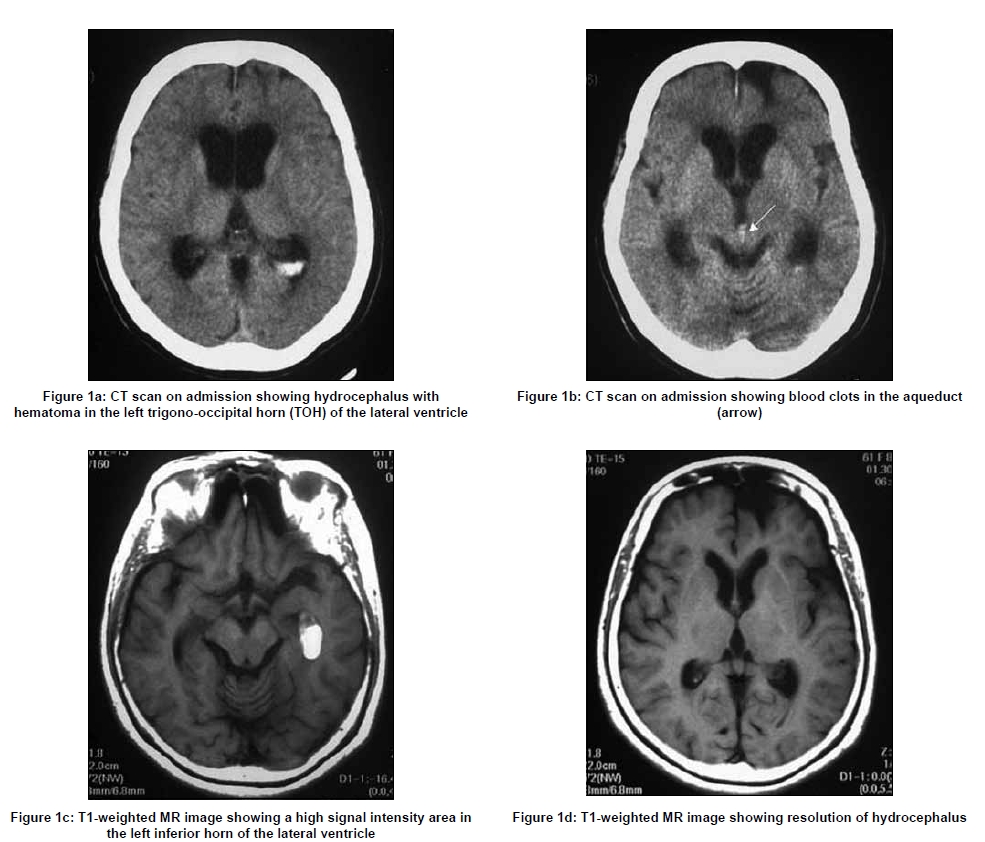
Correspondence Address: Department of Neurosurgery, Koyanagi Memorial Hospital, Saga Date of Acceptance: 05-Jun-2009 Code Number: ni09107 PMID: 19587490 DOI: 10.4103/0028-3886.53275 Sir, A 61-year-old female had an episode of headache lasting for three days. Findings upon physical examination were negative except for progressive disorientation. A computer tomography (CT) scan revealed intraventricular hematoma (IVH) in the left trigone and occipital horn, and hydrocephalus [Figure - 1]a and blood clots in the aqueduct [Figure - 1]b. As we suspected the presence of subarachnoid hemorrhage (SAH), we planned for an immediate magnetic resonance imaging (MRI). There was a waiting period for approximately 50 min between the initial CT scan and acquiring the MRI. During this period the patient was kept quiet in bed. MRI T1-weighted images done after 50 min of the initial CT scan showed temporal horn of the left lateral ventricle filled with a clot exhibiting high signal intensity [Figure - 1]c. MR images also revealed the resolution of hydrocephalus [Figure - 1]d. After MR imaging, she was more alert relieved of headache. No vascular anomaly was detected on MR angiography. She was discharged without neurological deficit. In our patient the initial CT scan showed left IVH in the tigone and occipital horn with obstructive hydrocephalus due to clot in the aqueduct. MRI done 50 min later showed resolution of hydrocephalus and blood in the temporal horn of the left lateral ventricle. For the period between CT scan and MRI, she was lying in the supine position. It was very unlikely for the clot to move from trigono-occipital horn (TOH) to the inferior horn of the lateral ventricle in this position. Spontaneous resolution of acute hydrocephalus without aspiration of cerebrospinal fluid (CSF) or drainage procedures is rare, and only a few cases have been reported previously. [1],[2] The presumed mechanism for the spontaneous resolution in these patients is aqueductal trapping and releasing of the clot. Cerebrospinal fluid dynamic in different types of hydrocephalus have been well studied. [3],[4],[5],[6],[7] We hypothesize the following possible mechanism for the spontaneous resolution of the hydrocephalus in our patient. Our patient had obstructive hydrocephalus secondary to the clot in the aqueduct with elevated intraventricular pressure. The blood clot in the left trigone and occipital horn might have resulted in the obstruction and entrapment of the left temporal horn leading to a significant elevation of pressure in the entrapped left temporal horn. We feel the pressure gradient between the entrapped left temporal horn and the rest of the ventricular system might have given a way in the blood clot located at the left trigone and occipital horn. This would have resulted in further increase in intraventricular pressure resulting in unplugging of the clot in the aqueduct leading to spontaneous resolution of the hydrocephalus. Subsequent to these events the clot in the left trigone and occipital horn might have slipped into the temporal horn. Our patient also demonstrates two other aspects: (1) the difficulty in identifying the cause of IVH and (2) how treatment strategies can change depending on the changes in the clinical status and investigative findings. Nomura [2] reported an interesting case in which hydrocephalus spontaneously improved six hours after onset due to movement of a clot plugging the aqueduct. However, it is very difficult to define the time window for unplugging of clot in the aqueduct in such cases. Resolution of the clot is likely to depend on the amount and location of the clot in the ventricle. The best approach in such patients would be to closely monitor the clinical status. If there is any deterioration in the level of consciousness, the therapeutic strategies, such as ventricular drainage or endoscopic removal of the clot should be instituted. We emphasize the importance of considering conservative management of hydrocephalus in a clinically stable patient with such clinical presentation. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09107f1.jpg] |
| |||||||||

{kind=link}