 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 4, July-August, 2009, pp. 387-394 Original Article Expression of VEGF and neural repair after alprostadil treatment in a rat model of sciatic nerve crush injury Jinrong Tang, Ye Hua, Jianhua Su, Ping Zhang, Xuejiang Zhu1, Le Wu2, Qi Niu, Hang Xiao2, Xinsheng Ding Departments of Neurology, 1Physiology and 2Neurotoxicology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, 210 029, China Correspondence Address: Prof. Xinsheng Ding, Department of Neurology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, 210029, China. dingxs6688@yahoo.com Date of Acceptance: 25-Jul-2009 Code Number: ni09115 PMID: 19770537 DOI: 10.4103/0028-3886.55583 Abstract Background: Vasoactive drug alprostadil improves microcirculation and can be effective in treating disorders of peripheral nerves. Vascular endothelial growth factor (VEGF) has been shown to have protective action in cerebral ischemia, disorders of spinal cord, and also peripheral nerves. However, the mechanism of action of VEGF in peripheral nerve injuries is uncertain. Keywords: Crush injury, dorsal root ganglion, sciatic nerve, vasoactive agent, vascular endothelium growth factor Introduction Crush injury to peripheral nerves can adversely affect neural microcirculation and capillary occlusion.[1] Consequently, ischemia and oxygen deficiency in nerves, destruction of the blood-nerve barrier, neural edema, disorder of the neural internal environment, and neural dystrophy appear, and can result in dysfunction of neural conduction. It has been reported by clinical and experimental studies that vasoactive treatment can alleviate the effects of lesions in peripheral nerves. [2],[3] Alprostadil is an effective agent for treating disorders of peripheral nerves. [4],[5],[6],[7] It is known that the vascular endothelial growth factor (VEGF) can protect against neuronal lesions. However, the changes in VEGF following crush injury to peripheral nerves, and the mechanisms of vasoactive treatment are incompletely understood. In order to explore the protective mechanisms involved in vasoactive treatment on peripheral nerves after injury, the sciatic nerves of rats were crushed, and the effect of the vasoactive agent, alprostadil, on expression of VEGF was assessed. Materials and Methods Sciatic nerve injury in rats After fasting for 12 hours, 400 sprague dawley (SD) rats (200 males and 200 females, SPF grade, body weight 180-220g, Shanghai Laboratory Animal Center, Shanghai, China) were randomly divided into: Control; saline; saline + VEGF antibody; alprostadil; and alprostadil + VEGF antibody groups. Each group included 80 rats (40 males and 40 females). All procedures were performed in accordance with the animal care guidelines of the Nanjing Medical University, which conform to the Guide for the Care and Use of Laboratory Animals (NIH publication No. 85-23, revised, 1985). The rats were fixed onto rat plates after they were anesthetized with 10ml/kg of 3% pentobarbital via intraperitoneal (ip) injection. An incision was made in the right hind limb to expose the sciatic nerve. [8] In the control group, the incision was closed after exposure of the sciatic nerve. The sciatic nerves of the rats in other groups were clipped using pressure equal to half of the body weight for 30s, the pressure was then released and the incisions were closed. Routine antibiotics were given to prevent infections. The rats in the alprostadil (Beijing Taide, batch number 2044T, Beijing, China) and VEGF antibody (Beijing Zhongsan Jinqiao Biotechnology Ltd., Beijing, China) groups were administered drugs (4 μg/kg/d, ip) and rabbit IgG polyclonal VEGF antibody (diluted with saline to 1:100, 2ml/d, ip), and an equivalent volume of saline (ip) was given to the rats in the saline group. Separation of dorsal root ganglia and sciatic nerve trunks The dorsal root ganglia (DRGs) and sciatic nerve trunks were separated immediately after the rats were sacrificed. The ribs were sheared along both sides of the spine, and the spine's thoracic and lumbar segments were removed. The section was cut along the median line, the spine segments, DRGs, neural roots and the sciatic nerve trunks were placed in culture dishes containing oxygen-enriched, saturated Dulbecco's Modified Eagle's Medium (DMEM), pH 7.4, the osmotic pressure was 340mOsm/L. DRGs, nerve roots (anterior and posterior roots) and the sciatic nerve trunks were removed from the neural canal. The membrane of the peripheral connective tissue, which connects to the nerve trunk, was removed under a stereoscopic microscope using fine corneal scissors, wire forceps and scissors. Detection of vascular endothelial growth factor mRNA in dorsal root ganglia cells The DRGs were taken at time points including: 0, 3, 6, 12, 24, 48, 72, and 96 hours, as well as at day seven after crushing the sciatic nerves. Reverse transcribed-polymerase chain reaction (RT-PCR) was performed as follows (reverse transcribed kit from Promega, Madison, WI, TRIzol from Invitrogen, Carlsbad, CA)
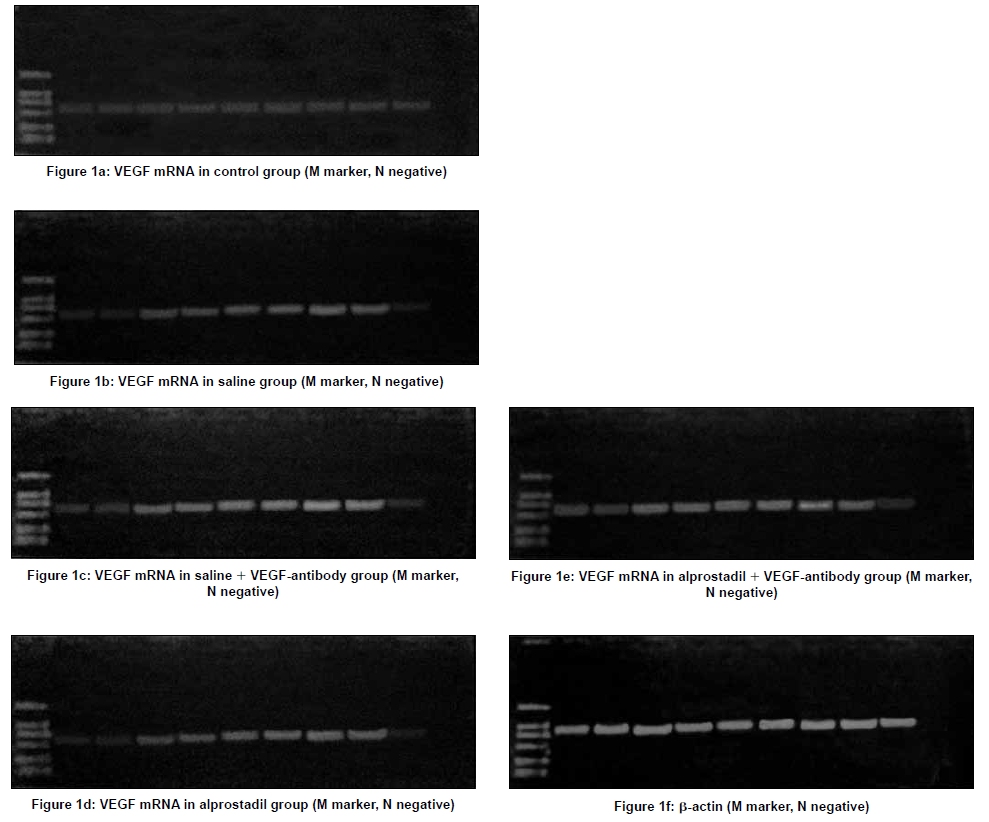
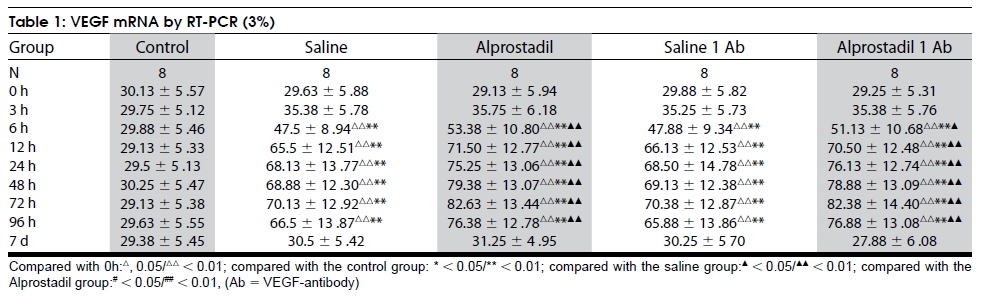
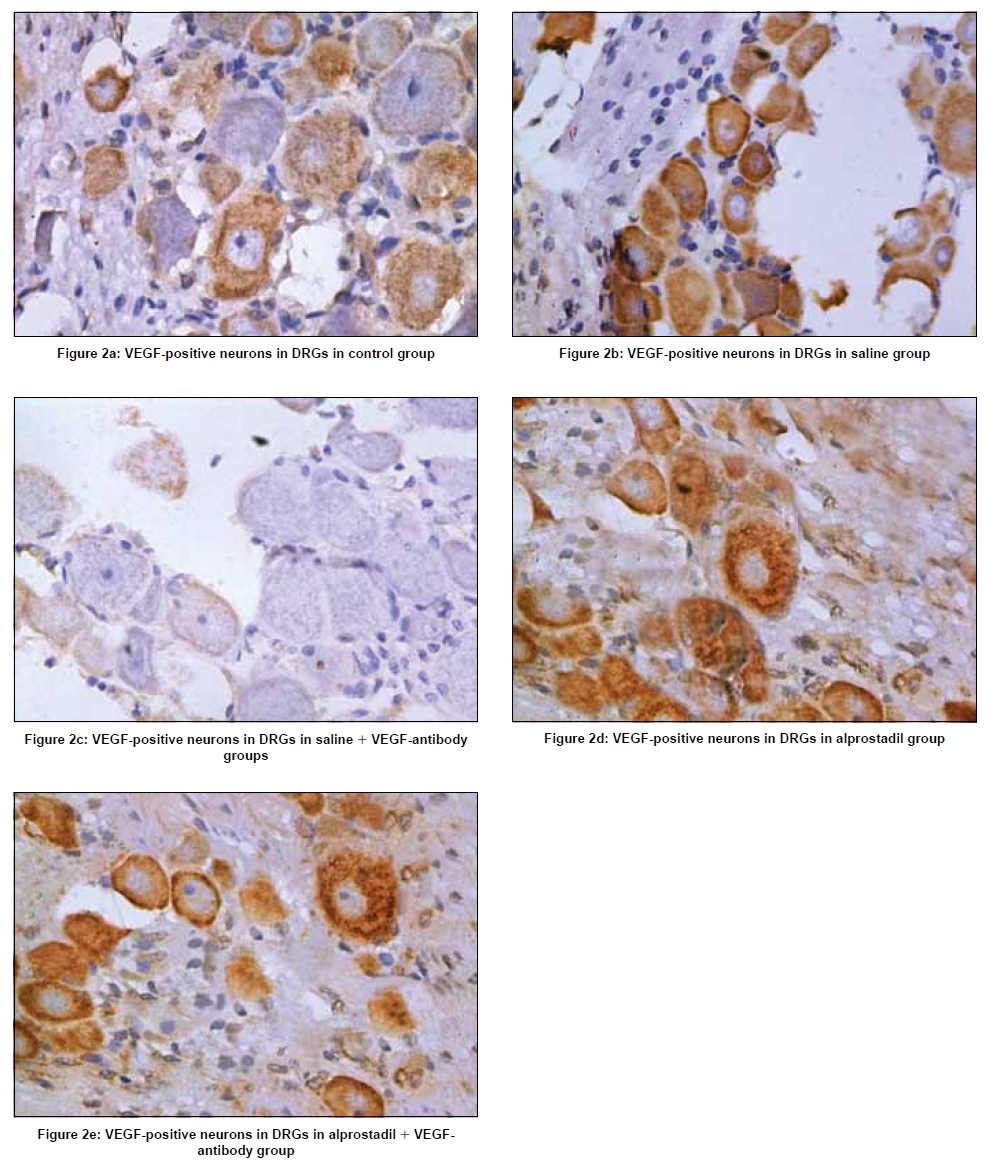
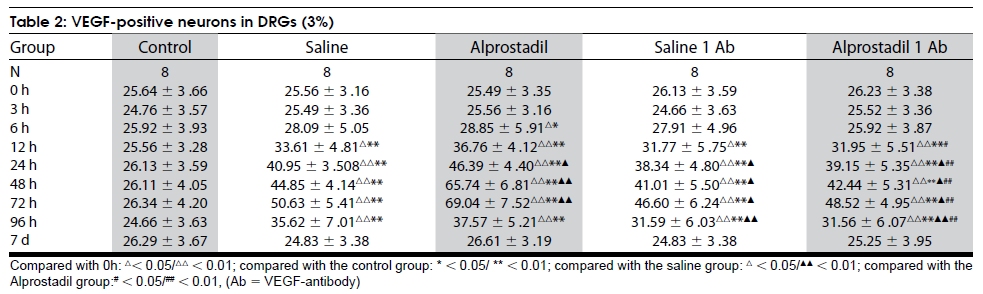
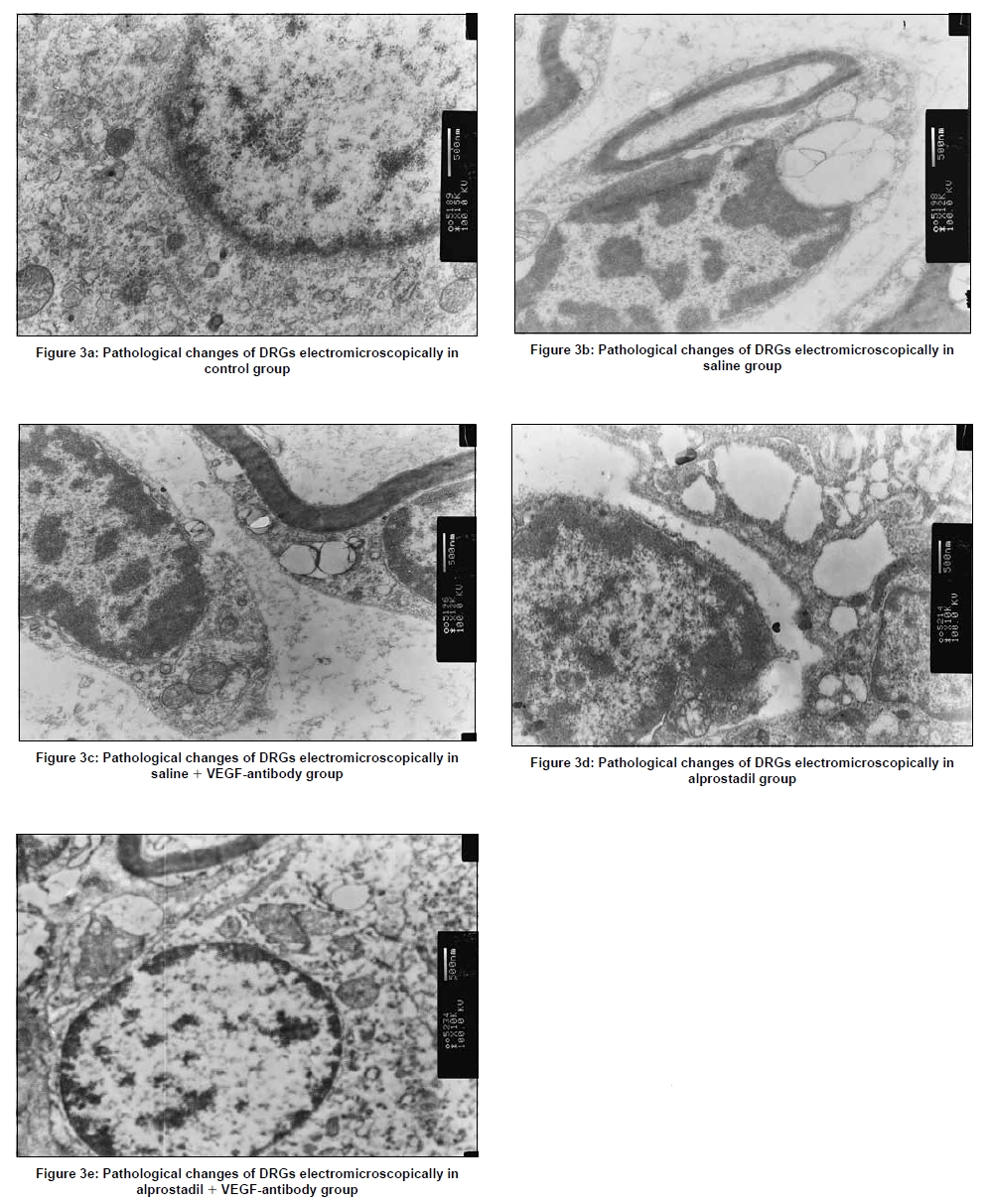
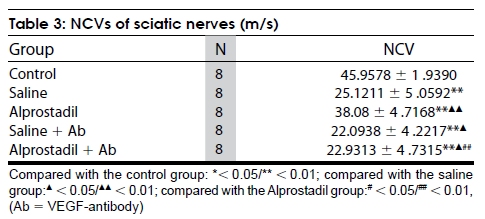
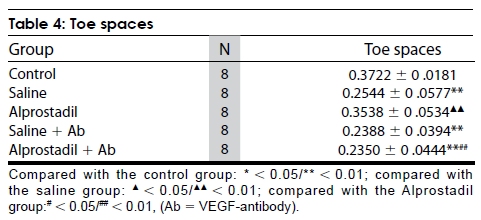
Detection of vascular endothelial growth factor positive neurons in dorsal root ganglia The DRGs of each group were taken at 0, 3, 6, 12, 24, 48, 72, 96 hours and day seven after crushing the sciatic nerves. They were treated as follows (pv-6001/6002 immunohistochemistry kit from Beijing Zhongsan Jinqiao Biotechnology Ltd. China): Immunohistochemistry (1) APES (3-aminopropyl triethoxysilane) smear was conducted on glass slides; (2) Routine deparaffinizing was performed on the sections; (3) The sections were incubated in 3% H 2 O 2 in deionized water for 5-10mins to block endogenous peroxidase; (4) Hot-fix of the antigens was performed; (5) The primary antibody (Immediate-use VEGF rat anti-human monoclonal antibody from the immediate-use non-biotin pv-6001/6002 reagent kit, Beijing Zhongshan Golden Bridge Biotechnology Co. Ltd. Beijing, China) was added. The sections were placed in 4°C refrigerator overnight and then rinsed with phosphate buffered saline (PBS) three times for 2mins each; (6) The secondary antibody (Immediate-use goat antimouse IgG-horse radish peroxidase (HRP) polymers from the immediate-use nonbiotin pv-6001/6002 reagent kit, Beijing Zhongshan Golden Bridge Biotechnology Co., Ltd.) was added. The sections were incubated at room temperature for 20-30mins, and then rinsed with PBS three times for 2mins each; (7) Diaminobenzidine (DAB) color development was conducted; (8) Washing with tap water was performed; (9) The samples were stained with hematoxylin, dehydrated, cleared and mounted. The sections were then observed under a microscope (50i, Nikon, Shanghai China) and the cells containing brown-yellow granules were considered to be positive. Image analysis Two specimens were randomly selected from each group at each time point and VEGF immunohistochemistry was performed. A light microscope (x400) was used to observe the number of cells with positive expression in each sample (five fields were randomly taken from each section to count the positive cells and the average value was calculated), and a comparison was conducted. Pathological examination The rats in each group were sacrificed at week four after crush. The DRGs and sciatic nerves were separated according to the method described. Examination of the DRGs and sciatic nerves was performed by electromicroscope. Nerve conduction velocities of sciatic nerves Eight rats from each group were killed at week four after crush. Then a 6-cm length of sciatic nerve trunk was separated. The Nerve conduction velocities (NCVs) of sciatic nerves in the NCV determination box (constant temperature 35ºC) were detected at 2mins, 3mins, and 4mins, respectively (D95Super Lab determinator of NCV from Medical Electrons Institute of Academe of Jiangsu Biomedical Engineering). Different parameters of a stimulus impulse were: 0.04ms, 2.7voltage, and scanner speed 50,000mm/s. The distance between the two recording electrodes on every sciatic nerve trunk was 3.5cm. The time of action potential peak of two recording electrodes was detected. Toe spaces The toe spaces of rats in each group were determined at week four after crush. We stained ink onto the rats' toes and made them walk on papers of 60cm length and 10cm width. The space of three to four toes of the right hind limbs was determined with vernier calipers. Statistics Statistical Package for the Social Sciences (SPSS, Bizinsight, Beijing China) 11.5 was used, and Pvalues < 0.05 were considered to be significant. Analysis of variance (ANOVA) was used for comparison. The number of spinal cord neurons and the number of cells expressing VEGF were consistent with normal distributions. The Student-Newman-Keuls analysis (SNK) method was used. Results Vascular endothelial growth factor mRNA by RT-PCR There was little expression of VEGF in all groups, 0h after crushing, and no significant difference among them ( P >0.05). Compared with 0h: (1) the VEGF mRNA levels were not different from the control group ( P >0.05); (2) VEGF mRNA from other groups increased at 3h and 6h ( P < 0.01 at 6h) after crushing, and the VEGF mRNA from the saline, saline + VEGF antibody, alprostadil and alprostadil + VEGF antibody groups at 6, 12, 24, 48, 72, and 96 hours were more than that at 0h ( P < 0.01); (3) VEGF mRNA peaked at 72h and then decreased to baseline, such that there was no difference between 0h and day seven in each group ( P > 0.05); (4) VEGF mRNA from the saline, saline + VEGF antibody, alprostadil and alprostadil + VEGF antibody groups were significantly more than that of the control group at 6, 12, 24, 48, 72, and 96hours ( P < 0.01); (5) VEGF mRNA from the alprostadil and alprostadil + VEGF antibody groups were significantly more than that of the saline group at 6, 12, 24, 48, 72, and 96 hours ( P < 0.05), but there was no intragroup difference ( P > 0.05). There was no difference between the saline1VEGF antibody group and the saline group ( P > 0.05) [Figure - 1],[Table - 1]. VEGF-positive neurons in DRGs There were only a few VEGF-positive neurons in the DRGs in the control group. In the alprostadil group, the number of VEGF-positive neurons began to increase at 6h ( P < 0.05), and at 12h in the other groups ( P < 0.01); the numbers peaked at 72h ( P < 0.01) and then started to decrease, returning to normal on day seven. The VEGF-positive neurons in the alprostadil group were more than that of the saline group at the same time ( P < 0.05). The VEGF-positive neurons in saline1VEGF antibody group were less than that of the saline group ( P < 0.05). The VEGF-positive neurons in the alprostadil + VEGF antibody group were less than that of the alprostadil group at the same time ( P < 0.05) [Figure - 2],[Table - 2]. Pathological changes of DRGs electromicroscopically In the saline and saline + VEGF-antibody groups, the density of electrons of numerous nuclei decreased, vacuolar degeneration and pyknosis appeared, the nucleoli or even nuclear structure disappeared, and the nuclear membrane was incomplete. The density of cytoplasm increased. The change of patching homogeneity, vacuolar degeneration, and many apoptosis body appeared in the cytoplasm. The pathological changes of the saline + VEGF-antibody group were more severe than those of saline group. In the alprostadil group, the density of electrons of some nuclei decreased and few apoptosis bodies appeared in the cytoplasm, and the other pathological changes were also less than those in the saline group. The pathological changes in alprostadil + VEGF-antibody group were severe than those in the alprostadil group. There was no pathological change of DRGs in the control group [Figure - 3]. NCVs of sciatic nerves The NCVs of sciatic nerves in the alprostadil group were faster than that in the saline group ( P < 0.05) and slower than that in the control group ( P < 0.01) at week four after crush injury. The NCVs of sciatic nerves in the saline1VEGF-antibody group were slower than that in the saline group ( P < 0.05) and the NCVs of sciatic nerves in the alprostadil + VEGF-antibody group was slower than that in the alprostadil group ( P < 0.05) at week four after crush injuries [Table - 3]. Toe spaces At week four after crush, the toe space in the saline group was significantly shorter than those in the control and alprostadil groups ( P < 0.01) and the toe space in the alprostadil group was not different to that in the control group ( P > 0.05). The toe space of the saline + VEGF-antibody group was shorter than that of the saline group, but there was no statistical value ( P > 0.05). The toe space of the alprostadil + VEGF-antibody group was shorter than that of the alprostadil group ( P < 0.01) [Table - 4]. Discussion Relevant research indicated that the expression of VEGF could be upregulated by anoxia. Following traumatic brain injury, there was an early (within 4h postinjury) increase in the expression of VEGF that was associated with neutrophilic invasion in the traumatized parenchyma. The maximum number of astrocytes expressing VEGF was observed on the fourth day after traumatic brain injury. [9] Macrophages in the periphery and the core of infarct represented the major source of VEGF during the early stages, 18h to day 2 postinjury. The number of immunoreactive macrophages decreased gradually from day 2, in both the periphery and core. VEGF was detected in neurons from 18h after the lesion to day five in the core, and up to day ten in the periphery. In the early stages, intracytoplasmic granular immunolabeling in the neurons and dendrites was observed. Immunostaining in glial cells was observed during the entire active period, from 18h after the lesion to day 14. However, their peak activities were occurred from day five to seven in the periphery. [10] Minamino reported that the expression of VEGF and other growth factors could be induced by hypoxia. [11] Gaumann found that the presence of VEGF was associated with tumor necrosis. Local hypoxia of tumors could induce VEGF and result in higher VEGFR-1 and VEGFR-2 levels in vascular endothelial cells. [12] Hypoxia increased the expression of VEGF mRNA and protein via the following mechanisms: (1) the regional promoter of VEGF included a response element of the hypoxia-inducible factor-1 (HIF-1). Hypoxia directly induced the expression of VEGF; (2) Stimulation of hypoxia activated c-Src, which increased the expression of VEGF; (3) During hypoxic induction, stability of VEGF was enhanced, and its half-life increased from 30-40min to 6-8h. This indicated that the increase in hypoxic-induced VEGF occurred on the transcriptional and post-transcriptional levels; (4) Mutations in the p53gene cause the survival of hypoxic tumors by increasing the expression of VEGF and decreasing the expression of thromboxane, and facilitating angiogenesis.[13] Vasoactive agents were commonly used in the clinic to treat crush injury to peripheral nerves, but the mechanism involved was unclear, until now. The results of this study demonstrated the vasoactive agent, alprostadil, could increase VEGF mRNA and VEGF-positive neurons in DRGs of rats after crush injury to sciatic nerves ( P < 0.05). Despite that VEGF mRNA expression was not affected by the VEGF antibody results in our study, the VEGF-positive neurons in the saline + VEGF antibody group was less than that of the saline group ( P < 0.05), and the VEGF-positive neurons in alprostadil + VEGF antibody group was less than that in the alprostadil group ( P < 0.01). This indicated that the number of the VEGF- plus VEGF receptor-positive DRG neurons increased with alprostadil treatment, but decreased when the VEGF antibody was used. This might be because the biological activity of VEGF was inactivated or decreased when combined with the VEGF antibody. Altogether this suggested that alprostadil could upregulate VEGF and increase the combined expression of VEGF and VEGF receptors in DRGs after crush injury to sciatic nerves. Whether the expression of VEGF alone or in combination with VEGF receptors in DRG neurons was upregulated in the alprostadil group, needs to be further confirmed. It has been shown that VEGF was a key mediator of the angiogenesis in ischemic lesions in nervous tissues.[14],[15],[16] Quattrini observed that VEGF-A staining was significantly reduced in diabetic patients, compared with control subjects in the upper dermis and on blood vessels, and was the lowest in cases of severe neuropathy. VEGFR-2 staining did not differ in the dermis, but was significantly reduced on blood vessels of diabetic patients with severe neuropathy, compared with control subjects and diabetic patients without neuropathy.[17] Zheng reported that systemic administration of recombinant VEGF significantly diminished astrogliosis and increased the number of neuromuscular junctions in a Cu/Zn superoxide dismutase (SOD1) transgenic mouse model of amyotrophic lateral sclerosis treated with saline. [18] Uesaka demonstrated that angiogenesis is essential for the enlargement of any solid tumor, and VEGF is considered to be a major regulator. [19] Aramoto found that VEGF could induce mild vasodilation and obvious increases in microvascular permeability. [20] Cooke reported that VEGF could stimulate the release of nitric oxide from cultured human umbilical venous endothelial cells and upregulate the expression of nitric oxide synthase. [21] Recent evidence suggested that VEGF was protective against the effects of lesions in neurons or nerves in brain ischemia, [14],[22],[23],[24] spinal cord disorders [25] and even impairment of peripheral nerves. [14],[25],[26] If the blood flow of neurotrophic vessels of nerve was reduced by crush injury to nerve, oedema appeared in nerve tissues due to oxygen deficiency, the volume of nerve tissues increased, the pressure in neurolemma increased, the microcirculatory disturbance was further aggravated, the crush of nerves was aggravated, and the dysfunction of neural metabolism and conduction occurred. [12] Li [27] found that when neurolemma was dissected during facial nerve decompression, the oedematous nerves would immediately bulge, the blood vessels of the epineurium became dilate, the color of the nerves turned from pale to red, and facial movement would recover dramatically. The results of pathology, NCVs and toe spaces in this experiment indicated that alprostadil could reduce the pathological injury and improve the functional recovery after crushing injury to sciatic nerves. This study indicated that when the expressions of VEGF and the number of the VEGF- plus VEGF receptor-positive DRG neurons increased with alprostadil treatment, the pathological lesion of DRGs was alleviated and the functional rehabilitation of sciatic nerves was accelerated. In addition, the benefit of alprostadil was decreased by application of VEGF-antibody. It was suggested that the overexpressions of VEGF was important in pathological and functional repair of crush injury to sciatic nerves by alprostadil treatment. Conclusions The results of this experiment indicate that the vasoactive agent alprostadil may reduce the pathological lesion of peripheral nerves and improve the rehabilitation of the neural function, which may relate to upregulation of the expression of VEGF, following crush injury to peripheral nerves. Acknowledgment This work was supported by the Medical Research Council [Grant number: Natural Science of Jiangsu Province BK2001116]. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09115t1.jpg] [ni09115t4.jpg] [ni09115t3.jpg] [ni09115f3.jpg] [ni09115t2.jpg] [ni09115f2.jpg] [ni09115f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}