 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
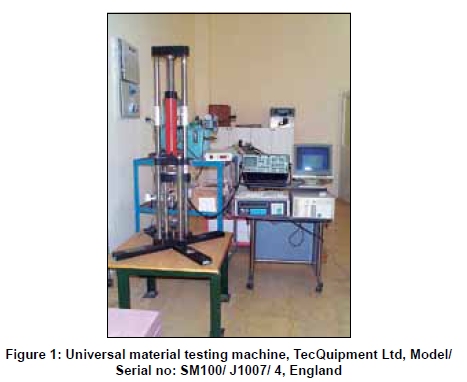
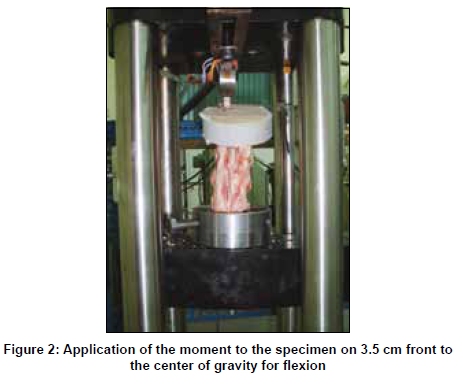
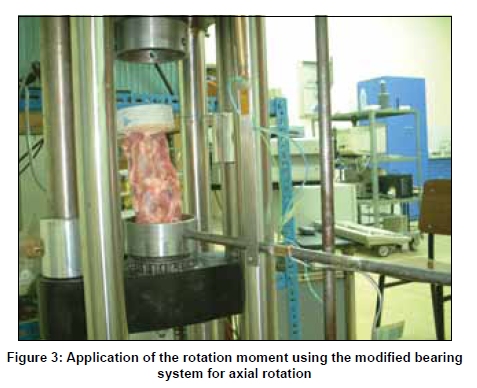
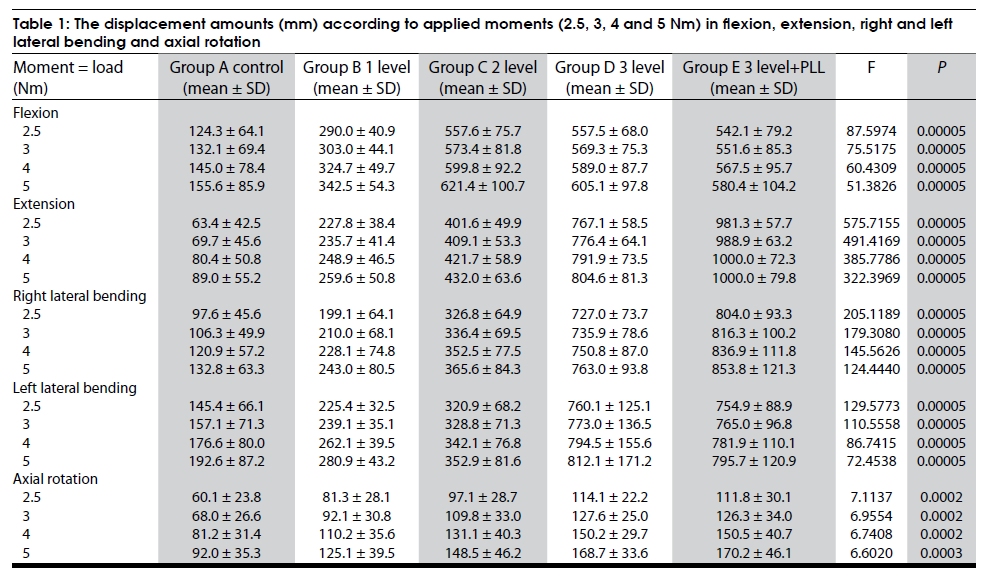
Neurology India, Vol. 57, No. 4, July-August, 2009, pp. 395-401 Original Article Biomechanical analysis of multilevel discectomy and excision of posterior longitudinal ligament: An in vitro study in sheep Cem Yilmaz, Serdar Kabatas, Kemal Hepgul1, Ergun Bozdag2, Emin Sunbuloglu2, Tufan Cansever Departments of Neurosurgery, Baskent University, Ankara, 1Faculty of Medicine, Istanbul University, 2Faculty of Mechanical Engineering, Istanbul Technical University, Istanbul, Turkey Correspondence Address: Dr. Serdar Kabatas, Department of Neurosurgery, Baskent University Istanbul Hospital, Oymaci Sokak No:7 34662, Altunizade, Istanbul, Turkey.kabatasserdar@hotmail. com Date of Acceptance: 02-Jul-2009 Code Number: ni09116 PMID: 19770538 DOI: 10.4103/0028-3886.55597 Abstract Aim: This experimental biomechanical study was performed to determine the effects of multilevel anterior cervical discectomy and excision of posterior longitudinal ligament (PLL) to stabilize the cervical spine using an in vitro animal model. Keywords: Animal model, biomechanics, cervical discectomy Introduction Since first introduced by Smith and Robinson [1] in 1955 and by Cloward [2] in 1957 an anterior approach to the cervical spine has gained wide acceptance by both neurosurgeons and orthopedic surgeons. The use of the anterior approach to remove herniated discs is safe and allows decompression of both the spinal cord and cervical nerve roots. Nevertheless, the intervertebral disc is of great importance in maintaining the stability of the spine. [3] Biomechanically, much of the focus on spinal stability has been on documenting the ability of the injured spine to maintain relationships between vertebrae through various mechanical tests. [4] Sophisticated knowledge of kinematic and biomechanical data is important to provide a useful guide in deciding the operative approaches for various cervical spine diseases and helps in preventing the potential late complications that can be caused by the biomechanical redistribution after treatment. [5] With this focus, we have aimed to evaluate whether anterior cervical discectomy affects stability or not using an in vitro sheep model. Materials and Methods Animal model The Animal Ethics and Research Committee of Istanbul University approved all protocols. A total of 50 three to four-year-old male merinos sheep weighing between 35 and 40kg were used for the study. Cervical spine pieces were excised by the surgeon immediately after the sheep were sacrificed. Care was taken not to damage ligamentous tissues while dissecting the spine pieces and physiological serum was used to moisten. [6] Spine pieces were moistened with physiological serum to prevent drying during the procedures and afterwards were wrapped with stretch films and preserved in -20 Celsius (°C) until the biomechanical tests were performed. [6],[7],[8] Experimental groups A total of 50 spine pieces (C3-6) were divided into five groups, each containing ten: Control group (A), one-level discectomy group (B), two-level discectomy group (C), three-level discectomy group (D), three-level discectomy and excision of posterior longitudinal ligament (PLL) group (E). Surgical procedure No surgery was carried out in Group A. For Group B one-level discectomy (C4-5), for Group C two-level discectomy (C3-4 and C4-5), for Group D and E three-level discectomy (C3-4, C4-5, C5-6) were performed. Discectomy procedures were performed by an anterior approach in groups B-E. The anterior longitudinal ligament (ALL) was incised in the midline and dissected from the vertebral bodies and the adherent annulus fibrosus (AF). The discectomies were performed by incising the annulus partially and then removing the nucleus and the remaining cartilaginous end plates with curettes and punches. Care was taken not to damage PLL except in Group E where ligament was excised. Biomechanical testing Biomechanical tests were performed in the Faculty of Mechanical Engineering of Istanbul Technical University. Standard static loading tests were used. [9] Specimens were non-destructively tested using a standard flexibility testing method. The pieces were thawed to room temperature and tests were performed in six hours. The upper half of C3 and lower half of C6 spines were fixed with polymethlymethacrylate in a PVC tube (Pimas, Gebze) 7.5cm in diameter and 2.2cm in height. All test specimens were fixated in normal lordotic alignment. Specimens were mounted in an electrohydrolic testing machine (Universal Material Testing Machine, Model/Serial No: SM 100/J1007/4, TecQuipment Ltd., England) and prepared for applying loads [Figure - 1]. A strain-gauge technique was used for measuring the displacements. This technique relies on the principle that an electrical conductor changes its electrical resistance when lengthening or shortening as a result of mechanical loads. Initially, in five specimens of the maximal loading group load deformation curves were obtained and minimal loading values causing disruption were determined for flexion, extension, right and left lateral bending, and axial rotation with one specimen for each movement. A load-cell with four strain gauges was constituted and a sliding system with minimal friction was used for flexion, extension, and lateral flexion. The moments were applied on 3.5 cm 2 front, back, right or left, respectively, to the center of gravity of the specimen [Figure - 2]. Unit shape changes (epsilon, E) were read from a strain-gauge bridge and a Data Logger (Model/Serial No: E31/J3080/3, Tecquipment Ltd., England,) and were transferred to a computer and recorded on a data system. These unit shape changes were recorded as moment according to the calibration values of the transducers and maximal loading moments were detected. Forces changing from zero to 3000 Newton (N) were applied. The displacements that occurred were recorded as unit shape change using a joint transducer made of a different stainless steel rod whose elasticity module, cross-sectional area and length is known and had been previously calibrated. For axial rotation a modified bearing system that could provide a rotation movement with minimal friction was located in the testing machine [Figure - 3]. This system did not allow any coupled motion. The inferior end of the spine piece was fixed and a series of moments changing from zero to 50 N were applied with a fixed velocity of 0.1 meter/second (m/s) to the superior end. The rotation that happened was recorded as epsilon with the help of the rod transducer that had been calibrated as degree. After finding the maximal loading values through this method, load deformation curves were drawn by loading from zero to five Newton-meter (Nm) for flexion, extension, right and left lateral bending and axial rotation in all groups. Five loadings were applied for each test. The first four were not taken into account in order to avoid visco-elastic effects and the curves were drawn according to the fifth test. Statistical evaluation To compare the control and discectomy groups, the displacements on 50 N were chosen for axial loading, and the data on 2.5, 3, 4 and 5 Nm were chosen for flexion, extension, lateral flexion on both sides, and axial rotation on both sides. The recorded data were taken to an x-y chart of moment versus displacement for each individual measurement on each specimen using Microsoft Excel. For each plot of the data, a third-order polynomial least-squares fit has been performed, and curves of R2 values of about 0.99 have been obtained for each single test. Then the corresponding displacement values have been recorded for 2.5, 3, 4 and 5 Nm loads grouped under each characteristic loading condition of the specimens for statistical analysis. One-way ANOVA was used to find out if there was difference between the groups for flexion, extension, right side bending, and axial rotation. A Levene test was made for the sensitivity of analysis of variants (homogeneity of variants). As the results of the analysis of variants showed that the groups were different from each other, a Bonferoni test was made to find out which groups were different from the others. For left side bending, as the homogeneity of the variants could not be proved by Levene test and ANOVA could not be applied. Kruskal-Wallis was applied as a non-parametric test. The groups were found to be different from each other as a result of the Kruskal Wallis test. A Mann-Whitney U-Wilcoxon W test was made in order to find which groups were different. A P value less than 0.05 was considered to be significant. Results Displacement amounts were determined for all seven movements. Results are shown in [Table - 1]. In statistical analysis, there were significant differences under 2.5, 3, 4 and 5 Nm moments between he five groups for flexion, extension, lateral bending in both sides and axial rotation. Results of statistical analysis are also shown in [Table - 1]. In flexion under 2.5, 3, 4 and 5 Nm, there were significant displacements in Group B (mean ± SD, 290.0±0.9, 303.0±44.1, 324.7±49.7, 342.5±54.3; 233, 229.5, 223.4, 220.1%, respectively) compared with Group A (mean±SD, 124.3±64.1, 132.1±69.4, 145.0±78 .4, 155.6±85.9, respectively, and Groups C, D and E mean ± SD, 557.6± 75.7, 573.4±81.8, 599.8±92.2, 621.4±100.7; (192.3,189.2, 184.7, 181.4%), respectively; 557.5 ± 68.0, 569.3±75.3, 589.0±87.7, 605.1±97.8; (192.2, 187.9, 181.4, 176.7%), respectively and 542.1± 79.2, 551.6±85.3, 567.5±95.7, 580.4±104.2; (187, 182, 175.1, 169.5%), respectively] compared with group B, ( P< 0.05). In extension under 2.5, 3, 4 and 5 Nm, there were significant displacements in Group B (mean±SD, 227.8±38 .4, 235.7±41.4, 248.9±46.5, 259.6±50.8; (359.3, 338.2, 309.6, 291.7%), respectively) compared with Group A (mean±SD, 63.4±42.5, 69.7±45.6, 80.4±50.8, 89.0±55.2, respectively), in Group C (mean±SD, 401.6±49.9, 409.1±53.3, 421.7±58.9, 432.0±63.6; (176.3, 173.6, 169.4, 166.4%), respectively) compared with Group B, Group D (mean±SD, 767.1±58.5, 776.4±64.1, 791.9±73.5, 804.6±81.3; (191.0, 189.8, 187.8, 186.2%), respectively) compared to Group C, and Group E (mean±SD, 981.3±57 .7, 988.9±63.2, 1000.0±72.3, 1000.0±79.8; (128, 127.4, 126.3, 124.3%), respectively) compared with Group D, ( P< 0.05). In right lateral bending under 2.5, 3, 4 and 5 Nm, there were significant displacements in Group B (mean ±SD, 199.1±64.1, 210.0±68.1, 228.1±74.8, 243.0 ±80.5; (204.0, 197.5, 188.7, 183.0%), respectively) compared with Group A (mean±SD, 97.6±45.6, 106.3±49.9, 120.9±57.2, 132.8±63.3, respectively), in Group C (mean±SD, 326.8±64.9, 336.4±69.5, 352.5±77.5, 365.6±84.3; (%164.1, 160.2, 154.5, 166.4), respectively) compared to Group B, and in Groups D (mean±SD, 727.0±73.7, 735.9±78.6, 750.8±87.0, 763.0±93.8, (222.4,218.7, 213, 208.7%), respectively) and E (mean±SD, 804.0±93.3, 816.3±100.2, 836.9±111.8, 853.8±(121.3; %246.0, 242.7, 237.4, 233.5), respectively) compared with Group C, ( P< 0.05). In left lateral bending under 2.5, 3, 4 and 5 Nm, there were significant displacements in Group B (mean±SD, 225.4±32.5, 239.1±35.1, 262.1±39.5, 280.9±43.2; (155.0, 152.6, 148.4, 145.8%), respectively) compared with Group A (mean±SD, 145.4±66.1, 157.1±71.3, 176.6±80.0, 192.6±87.2, respectively), in Group C (mean±SD, 320.9±68.2, 328.8±71.3, 342.1±76.8, 352.9±81.6; (142.4, 160.1, 130.5, 125.6%), respectively) compared with Group B, in Groups D (mean±SD, 760.1±125.1, 773.0±136.5, 794.5±155.6, 812.1±171.2 (236.9, 235.2, 232.2, 230.1%), respectively) and E (mean±SD, 754.9±88.9, 765.0±96.8, 781.9±110.1, 795.7±120.9; (235.2, 232.6, 228.5, 225.5%), respectively) compared with Group C, ( P< 0.05). In axial rotation under 2.5, 3, 4 and 5 Nm, there were significant displacements in Group C (mean±SD, 97.1±28.7, 109.8±33.0, 131.1±40.3, 148.5±46.2; (161.6, 161.5, 161.4, 161.4%), respectively), Group D (mean±SD, 114.1±22.2, 127.6±25.0, 150.2±29.7, 168.7±33.6; (189.9, 187.6, 184.9, 183.4%), respectively), and Group E (mean±SD, 111.8±30.1, 126.3±34.0, 150.5±40.7, 170.2±46.1; (186.0, 185.7, 185.3, 185%), respectively) compared with Group A (mean±SD, 60.1±23.8, 68.0±26.6, 81.2±31 .4, 92.0±35.3, respectively), ( P< 0.05). Discussion In patients who have failed conservative treatment, anterior cervical discectomy and fusion (ACDF) is an established procedure for the management of cervical neck pain, radiculopathy and myelopathy. However, a gold standard for the treatment of degenerative disc disease has not been identified in the recent literature. [10] Theoretically, fusion relieves neural irritation by immobilizing the spine and resorption of osteophytes. Indeed, use of bone grafts increases fusion rate, but fusion rates can be low in multilevel discectomies. Jacops et al . stated that discectomy alone has a shorter operation time, hospital stay, and postoperative absence from work than discectomy with fusion, while there is no statistical difference for pain relief and rate of fusion. [11] As the most important component in the structure and function of the human spine, the intervertebral disc is of great importance in maintaining the stability of the spine. It is generally accepted that disc degeneration contributes to the risk of spinal instability. [3] This study suggested that discectomy redistributed the mobility both at the discectomied and adjacent motion segments similar to recent literature. [5] Located on the radial periphery of the intervertebral disc, the AF is believed to experience a combination of compressive, tensile and shear stresses during weight-bearing and intervertebral joint motions. [12] One of the limitations of this study was that after the discectomy procedure the AF may cause pseudoinstability due to its relaxation. Additionally, resection of PLL may cause cervical instability. In Group E where PLL was excised, displacement increased in all ways, but it was significant in extension. The PLL is one of the important structures limiting flexion. PLL which is part of the middle column of Denis was thought to be effective in maintaining stability. [6],[7] Therefore, it must be evaluated by a separate study if PLL resection causes instability in cases in whom different level discectomies (e.g., one) are performed. In the present study, we only tested PLL resection in three-level discectomies. There has been much controversy about defining and diagnosing spinal instability. Segmental instability is generally defined as greater displacement between vertebrae under physiologic load. [3] However in biomechanics, diverse parameters have been developed as indicators of system stability or robustness. [13] The basic element in biomechanical studies is motion segments. A motion segment consists of two adjacent vertebrae and ligaments that join these. As the spine is not homogenous, the results obtained by examining motion segments cannot be generalized to the whole spine. Furthermore, the movements of the whole spine do not occur in isolation, but as combinations called coupling. More physiological results can be obtained by this way, but as coupling occurs when a long spine segment is used, this makes the study out of control and subjects it to the effects of biological variations. To prevent this, we used short motion segments and to prevent coupling when moment was applied in flexion, extension, right and left lateral bending, we used a sled system with minimum friction. [14] Additionally, different testing methods have been used to study cervical spine biomechanics, the two most common ones are load or displacement control. [15] In a recent study, DiAngelo and Foley suggested that a biomechanical testing apparatus can be controlled under load, displacement, or a hybrid control. [16] We therefore controlled both load and displacement in a relevant biomechanical testing apparatus. In a group of studies comparing simple discectomy and discectomy with fusion, human cadaver models were used. [17],[18] Schulte et al . biomechanically tested the immediate kinematic changes after discectomy without bone grafts. [17] The result of this study show that, the range of motion (ROM) was increased in flexion, extension, lateral bending and axial rotation. After using a bone graft, the ROM decreased in extension, lateral bending, and axial rotation. The most important problem here is that living tissue can show different resistance to loading by time and biomechanical evaluation immediately after the operation has low clinical applicability. [7],[17],[19] The disadvantages of in vitro human cadaver models are: They are hard to obtain, they are expensive, and show much variability. [20] In our study, we preferred to use in vitro animal model because it is easy to obtain, inexpensive, and didn't show much variability. It keeps its head straight most of the time and shows similarity to the human spine biomechanically. Moreover, there are experimental studies showing that sheep cervical spine is an appropriate model for humans both biomechanically and anatomically. [21],[22] On the other hand, the cervical spine is a complex mechanical system with many degrees of freedom. The multiple muscles of the cervical spine act to support and move the head in three-dimensional space. [23] Thus, cervical muscle is crucial in providing the stability of the cervical spine.[24] Modeling by Van Ee et al . demonstrated that muscle activation affects the level most apt to be injured and the loads at which failure occurs. [25] Nevertheless, the role of the paraspinal muscles, which play a dynamic role in controlling the alignment of the cervical spine, has not been evaluated in in vitro studies. Active musculature, which was unable to be modeled in this study, may also affect the mechanical response of these tissues. The peak moment magnitudes are different in human cadaver cervical spine models. Goel et al . tested at the lowest moment of 0.3 Nm, in latter studies 1.8 Nm (Moroney et al . and Pelker et al .), 4.5 Nm (Wen et al .) levels were tested. [26] Thus, we preferred to apply 2.5, 3, 4 and 5 Nm to test different levels in the same model. Spinal levels used in the testing protocol are also different. Moroney et al . and Wen et al . tested single-level functional units; Lysell, and Goel et al . tested C2-T1 columns; Panjabi et al . tested two-level functional units or multilevel columns; and Richter et al. tested three-level motion segments. [26] In our study, we used C3-C6 column which was a more relevant model to be tested. In the present study, all control group displacement amounts were similar to the previous study (e.g., 124.3±64.1 Nmm displacement in flexion under 2.5 Nm). [9],[27] With respect to these findings, we first investigated a statistically significant difference in displacement amounts between control and both discectomy groups. Furthermore, we determined excessive percentile loss of the cervical stability between the one-level discectomy group and multilevel discectomy groups ( P< 0.05). In Group B, one-level discectomy achieved slightly more stability on flexion motion (e.g., 233% displacement under 2.5 Nm) compared to multilevel discectomy groups (e.g., 448.6% under 2.5 Nm in Group C). For Groups C, D and E, the percentile changes of cervical spine over time were reliable results related to increases in the motion range of flexion load. [5] We additionally identified that there were significant displacements in extension in all groups ( P< 0.05). Regarding anterior discectomies decrease the stress absorption at the motion segments and directly transmit the physiological loads onto contiguous motion segments. [5] This effect superposed on the limitation of motion segments in extension load may cause a compensatory increase in extension motion range of the contiguous motion segment. Consistent with our data, the biomechanical reports also showed discectomy causes instability in ACDF biomechanical/clinical models. [28] The other changed variable of the results is that an increase in the displacement amounts of right/ left lateral bending was observed in the present study ( P< 0.05). Nevertheless, some authors stated that discectomy had the least impact on lateral bending. [28] However, more reliable studies concerning right or left lateral bending must be performed on human cadavers because of the fact that uncovertebral joints that limit lateral flexion are not present in sheep. Lastly, we observed marked percentile loss of the cervical stability between multilevel discectomy groups and control group in axial rotation. In Group B, one-level discectomy showed slightly similar results as control group (e.g., 81.3±28 .1 Nmm in Group B and 60.1±23 .8 Nmm under 2.5 Nm). Nevertheless, in a recent study performed in C2-4 levels, discectomy showed an increased motion range at both the C2-C3 and C3-C4 motion segments. [5] In the present study, we determined excessive percentile loss of the cervical stability in all segments ( P< 0.05). Together, our data support the opinion that cervical discectomy causes cervical instability. Conclusion A set of quantitative data of the displacement amounts and percentile loss of the sheep cervical spine has been reported. Related to the amount of variation between one, two and three-level discectomy decreases stability of sheep spine pieces. These data may have provided clinical relevance regarding the role of the biomechanical response for cervical spine after discectomy procedures. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09116f2.jpg] [ni09116t1.jpg] [ni09116f1.jpg] [ni09116f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}