 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
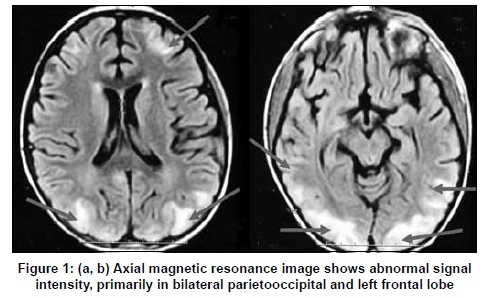
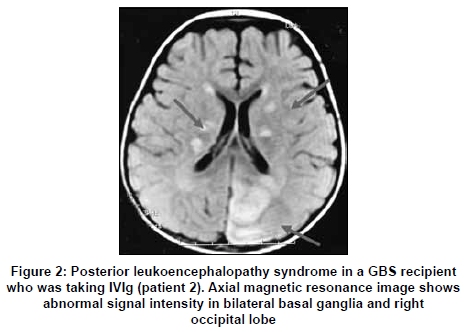
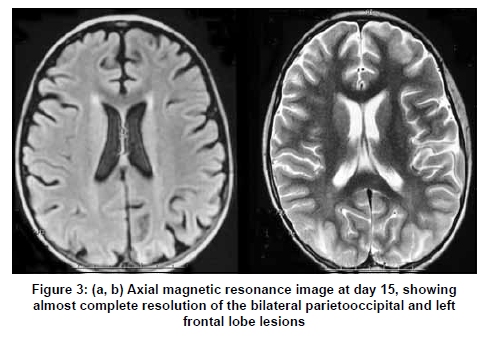
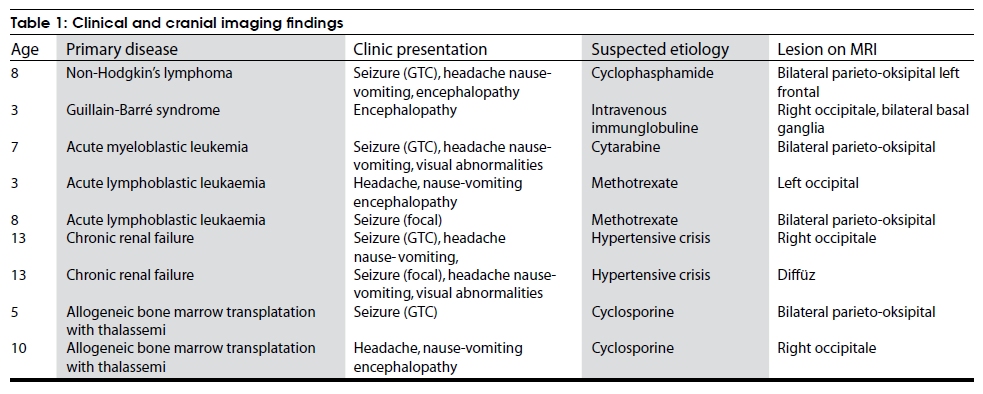
Neurology India, Vol. 57, No. 4, July-August, 2009, pp. 475-478 Brief Report Evaluation of nine children with reversible posterior encephalopathy syndrome Faruk Incecik, M. Ozlem Hergüner, Sakir Altunbasak, Fatih Erbey1, Goksel Leblebisatan2 Departments of Pediatric Neurology, 1Pediatric Oncology, and 2Pediatric Hematology, Cukurova University Medical Faculty, Adana, Turkey Correspondence Address: Dr. Faruk Incecik, Toros mah, 40 Sok, Omer Bayram Havus Apt., Kat: 11, No: 11, Adana, Turkey. fincecik@yahoo.com Date of Acceptance: 02-Jul-2009 Code Number: ni09131 PMID: 19770551 DOI: 10.4103/0028-3886.55605 Abstract Background: Reversible posterior leukoencephalopathy syndrome (PRES) is a neurological disorder characterized by signs of posterior cerebral edema upon radiographic examination. Keywords: Children, clinical and radiological findings, reversible posterior leukoencephalopathy syndrome Introduction Reversible posterior leukoencephalopathy syndrome (PRES) is a clinical and radiological syndrome, first described by Hinchey et al. in 1996. [1] The main causes of this condition include hypertensive crisis, renal failure, fluid retention, and some immunosuppressive drugs. But, it has recently been identified in a wide variety of conditions, including posttransplantation stage of liver diseases, acute chest syndrome in sickle cell disease, hemolyticuremic syndrome, acute intermittent porphyria, malignancies, vasculitis, eclampsia, transfusion, and erythropoietin, oxybutynin or intravenous immunoglobulin (IVIg) treatment. [2],[3],[4],[5] The most common clinical manifestations of PRES are seizures, headache, nausea and vomiting, altered mental status, decreased alertness, cortical blindness, and transient motor deficits. The main finding in neuroimaging is posterior white matter oedema, which is predominating in the occipital and parietal lobes and posterior fossa structures. [1] In this study, we evaluated clinical and radiological findings in nine children who were diagnosed with PRES. Materials and Methods We retrospectively analyzed the records of nine children with the diagnosis of PRES between January 2006 and June 2008 at the University of Cukurova Hospital, Turkey. Diagnostic criteria for PRES included an increased diffusion coefficient in regions of T2 hyperdensities on diffusion-weighted imaging (DWI) with associated symptoms of neurological alterations such as headache, loss of consciousness or seizures. Data were collected on their age at presentation, gender, symptoms, physical and neurological examination findings, radiological findings, and primary underlying etiology. All of the magnetic resonance imaging (MRI) and electroencephalography (EEG) studies were also completed within the first 24-48 h of presentation. MRI was performed with a 1.5-T scanner and precontrast imaging sequences [T1-weighted, T2-weighted, and fluid-attenuated inversion recovery (FLAIR)] and postcontrast T1-weighted images were also obtained. Arterial blood pressure was monitored in all patients and serum biochemistry panel was obtained. Results We identified nine patients (seven boys and two girls), who had the characteristic clinical and imaging features of PRES. The mean age of the children was 7.78±3.76 years (range 3-13 years). The primary etiology, in two patients was taking intrathecal methotrexate for acute lymphoblastic leukaemia (ALL-L2), in another two patients was taking cyclosporine for allogeneic bone marrow transplantation for thalassemia, in one patient was taking intrathecal cytarabine (Ara-C) for acute myeloblastic leukemia (AML), in one patient was taking cyclophasphamide for nonHodgkin's lymphoma, in one patient was taking IVIg for Guillain Barre syndrome (GBS), and the last two patients had chronic renal failure and acute hypertensive crisis. The most presenting symptoms were seizure, headache and altered consciousness. Six patients had seizures. Four of these had generalized tonic-clonic seizures (GTC), and two had focal seizures. Altered consciousness was present in only four patients. Headache and nausea or vomiting was present in six patients. Visual abnormalities were noted in two patients, consisted of blurred vision. These signs and symptoms resolved after discontinuing of immunosuppressive drugs and IVIg in seven cases, and after starting antihypertensive management in two cases. The median time to clinical resolution was four days (range, 2-12 days). The most common location of the white-matter abnormalities on MRI was in the posterior regions of the cerebral hemispheres [[Figure - 1]a and b; patient 1]. Isolated parietal and occipital involvement was noted in six patients. We showed involvement of frontal lobe in two patients, temporal lobe in one patient, cerebellar in one patient, and basal ganglia in one patient on MRI [[Figure - 2]; patient 2]. These abnormalities were bilaterally symmetric in five cases and asymmetric in the other five patients. In follow-up, one month later, neuroimaging changes had disappeared or almost completely resolved in all of the patients [[Figure - 3]a and b; patient 1]. EEGs were obtained for only seven of them; diffuse slowing activity was observed in two patients and normal in five patients. Clinical and neuroimaging findings are summarized in [Table - 1]. Discussion The most common clinical manifestations of PRES are headache, nausea and vomiting, altered mental status, decreased alertness, seizures, cortical blindness, and transient motor deficits. In the patients with PRES, seizures are common at the onset of neurologic symptoms but can also develop later. The seizures are usually GTC type and multiple. Temporary restlessness and agitation may alternate with lethargy. Stupor and coma may develop. The patients are often confused and there may be some abnormalities of vision such as hemianopia, blurred vision, and cortical blindness. [2],[6] In previous reports of PRES, all of these clinical features do not describe in all pediatric PRES patients. In a study of 25 children with PRES, 44% manifested all four clinical signs or symptoms, 32% demonstrated three, 16% had two, and 8% had only one sign or symptom. [7] Kwon et al . [2] reported 12 patients who presented with seizures (42%), visual disturbances (33%), headache (17%), or altered mental status (8%). In all of our patients, we detected the most common clinical features as seizure (6/9), headache (6/9), and altered consciousness (4/9). The other symptoms were nausea and vomiting and blurred vision. Many predisposing factors have been proposed including hypertension, immunosuppressive drugs, eclampsia, and renal dysfunction. But, there were some differences in the etiological factors between the children and the adults, as in the clinical features. Hypertension has often been emphasized as a common feature of PRES-associated conditions. [1] PRES related to hypertension might be due to sudden elevation of blood pressure causing disruption of the autoregulatory mechanisms of the central nervous system vasculature, leading to vasoconstriction and vasodilatation, and breakdown of the blood-brain barrier.[8],[9] Onder et al . [8] detected hypertensive crisis as the most common trigger of PRES in 59%. In our patients, only two of the nine PRES patients had chronic renal failure and hypertensive crisis. The causes of chronic renal failure were focal segmental glomerulosclerosis and membranoproliferative glomerulonephritis. Although hypertensive encephalopathy is the most common cause of PRES, cases have occurred in the absence of severe hypertension. Renal dysfunction also appears to predispose to PRES, because of chronic uremia or fluid overload. Considering the rare frequency of arteriosclerosis and good plasticity of vessel walls in children, the vulnerability of vessel walls to hypertension was decreased in childhood. [4] Posterior leukoencephalopathy syndrome is also obscure during treatment with immunosuppressive and cytotoxic drugs. [1],[2],[3],[4] These drugs may have a direct cytotoxic effect on vascular endothelial cells. Direct toxic effects on the vascular endothelium can produce damage to the blood-brain barrier. The immunosuppressive and cytotoxic drugs may induce and exacerbate hypertension and may lower seizure threshold. Intrathecal chemotherapy may cause cerebral vasospasm, contributing to cerebral vascular autoregulation impairment. [4],[6],[10] Our patients were treated with intrathecal methotrexate, cytarabine, cyclophasphamide, cyclosporine and IVIg for ALL-L2, AML, nonHodgkin's lymphoma allogeneic bone marrow transplatation, with thalassemia and GBS, respectively. Importantly, seven children were normotensive and were not hypertensive at presentation and follow up. We have detected hypertension only in two patients with chronic renal failure. We were discontiuned the immunosuppressive drugs and IVIg treatment in seven of them, and began the antihypertensive management in two hypertensive patients. PRES resolved morly completely in all of the patients. In hypertensive patients, after the antihypertensive treatment, both patients recovered completely. In a previously report, characteristic findings of PRES on MRI have been well identified. [1],[2],[3] The MRI findings include oedema involving the white matter in the posterior regions of the cerebral hemispheres, especially bilaterally in the parietooccipital regions. Changes in the gray matter, cerebellum, and brainstem have also been described. [1],[8],[11] MRI shows hypotense lesions within the posterior white-matter regions on T1, and hyperintense signal on T2-weighted and FLAIR images. DWI reveals increased diffusion in affected regions, suggesting vasogenic oedema in these areas. The preferential involvement of the parietal and occipital lobes is hypothesized to be related to the less dense sympathetic nervous system innervation of the posterior cerebral circulation. [12] On MRI studies, DWI and apparent diffusion coefficient (ADC) imaging might be more sensitive for only diagnosis. In our patients, the brain MRI were studied in all of them and revealed typical radiologic changes typical of PRES. Parietal and/or occipital lobe involvement was present in all patients. We also obtained isolated parietal and occipital involvement in six patients. As a conclusion, the causes of the PRES may be multifactorial. It is important to consider this diagnosis in children presenting with encephalopathy and seizures in an appropriate clinical settings. Because, the clinical features and neuroimaging findings usually disappear after starting appropriate treatment or discontinuing or dose reducing of the immunosuppressive drugs and with this situation recovery almost completely in the patients with PRES. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09131t1.jpg] [ni09131f3.jpg] [ni09131f2.jpg] [ni09131f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}