 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
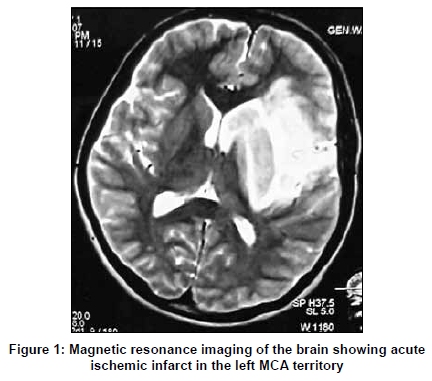
Neurology India, Vol. 57, No. 4, July-August, 2009, pp. 479-480 Case Report Acute ischemic infarct in the middle cerebral artery territory following a Russell's viper bite Sanjeev K. Narang, Srikanth Paleti, M. A. Azeez Asad, Tarannum Samina Department of General Medicine, Mamata General Hospital, Mamata Medical College, Khammam, Andhra Pradesh, India Correspondence Address: Dr. Sanjeev K. Narang 10-2-107, SVPD, Mamillagudem, Khammam, Andhra Pradesh, India. narang_sanjeev@yahoo.com Date of Acceptance: 26-Feb-2009 Code Number: ni09132 PMID: 19770552 DOI: 10.4103/0028-3886.55594 Abstract Ischemic stroke following snake bite is rare. We report an 18-year male who developed right hemiplegia with expressive aphasia following a Russell's viper bite. T2-weighted magnetic resonance imaging revealed infarct in the left middle cerebral artery territory. The possible mechanisms for cerebral infarction in this scenario include disseminated intravascular coagulation, toxin induced vasculitis and endothelial damage.Keywords: Cerebral infarct, Russell's viper, snake bite Introduction In India more than 20,00,000 snake bites are reported annually, of which 35,000 to 50,000 people die. [1] Russell's viper, Vipera russelli siamensis, is the leading cause of fatal snake bite in India. [2] The clinical characteristics include local cellulitis, renal failure, and hemorrhagic manifestations including pituitary and intracranial hemorrhage. In this report we present an unusual complication, cerebral infarction following Russell's viper bite. Case Report An 18-year-old previously healthy male was admitted for a snake bite on his left foot which he sustained in his paddy fields. The killed snake was identified as Russell's viper. He complained of severe pain. Local examination showed two deep fang marks, erythema and edema. Neurological examination was essentially normal on admission. He was immediately treated with 30ml loading dose of equine polyvalent antisnake venom (ASV-ASIA, Bharat Serum and Vaccines Ltd.) after a test dose, followed by continuous intravenous administration of 30ml every 6 hours by syringe pump until clotting time normalized. A further dose of 30ml over 24 hours was given to prevent recurrence of abnormal coagulation profile. [3] An injection of adsorbed tetanus toxoid was also given. Laboratory investigations: Mild leukocytosis, microscopic hematuria, prolonged bleeding time (5.00min) and clotting time (12:00min), prolonged prothrombin time (.3min; control 16sec) and activated plasma thromboplastin time (.180sec; control 36sec). Serum fibrinogen was 0.2g/dL and fibrin degradation products were negative. Clotting time was corrected in about 24 hours. Prothrombin time and activated plasma thromboplastin time were normalized by the fourth day. On the second day of the bite, patient developed right side weakness and speech disturbances. Neurological examination revealed right hemiplegia and expressive aphasia. Brain computed tomography (CT) scan and magnetic resonance imaging (MRI) showed acute ischemic infarct in the left middle cerebral artery territory [Figure - 1]. Magnetic resonance angiography of the cerebral circulation revealed no abnormalities. Colour Doppler study showed no arterial or venous thrombosis in the lower limbs. Work-up for other stroke risk profiles electrocardiogram (ECG), lipid profile including lipoprotein (a), serum homocystiene, proteins C, S, and antithrombin III, carotid Doppler and 2D echocardiography were normal. Patient showed improvement in the motor power and speech at the time of discharge on the tenth day. At 14-months follow-up he had good functional recovery and is able to carry activities of daily living with little difficulty, modified Rankin score 1. Discussion Cerebral complications, particularly ischemic complications, after snake bite are rare. Very few cases of cerebral infarction resulting from a viper bite have been reported. [4],[5],[6] In a study of 309 patients with snake bite, Mosquera, et al . reported cerebrovascular complications in 8 patients (2.6%), 7 hemorrhagic strokes and 1 ischemic stroke. [4] Bashir and Jinkins reported a patient in whom envenomation with Russell's viper resulted in hemiplegia and aphasia, consistent with a middle cerebral artery infarction. [5] Murthy, et al. reported a case of cerebral infarction and diffuse encephalopathy following a viper bite. [6] Viper snake venom is a complex toxin with rich components dominantly affecting hemostatic mechanisms. [7] In large doses, it can cause massive intravascular coagulation leading to small and even large vessel occlusions resulting in cerebral infarction. [8] Toxic vasculitis caused by certain viperine species may result in thrombosis. [6] Bashir and Jinkins suggested direct action of the venom on vascular endothelial cells. [5] Hemorrhagins, the complement mediated, toxic components of Viperidae snake venom may result in severe vascular spasm, endothelial damage, and increased vascular permeability, [5] all of which may contribute to vascular occlusion. [6] Hypercoagulation due to procoagulants in the venom, such as arginine, esterase, and hydrolase [5],[6] and hyperviscosity caused by hypovolemia and hypoperfusion secondary to hypotension may also contribute to vessel occlusion. The cerebral infarction may be totally unrelated and may be the manifestation of an inherent deficiency of protein C, protein S, and antithrombin III. [9] Our patient was young and had no vascular risk factor and MR angiography was normal. We feel in our patient the cerebral infarction was the result of toxic vasculitis or toxin induced vascular spasm and endothelial damage. Better outcomes have been reported with immediate ASV treatment. In the study by Thomas et al. , of the 33 patients with envenomation by Bothrops lanceolatus who had not received ASV or received ASV after 8 hours of envenomation, 14% developed thrombotic complications and 4 of the 14 patients who had not received ASV died. Of the 70 patients who received ASV within 6 hours of envenomation, none thrombotic complications. [ 10] Our patient, despite treatment with ASV within 1 hour of envenomation developed delayed cerebral infarction on the second day. Our case also illustrates that one should work up for possible cerebral infarction in a victim of viper envenomation and focal deficit. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09132f1.jpg] |
| |||||||||

{kind=link}