 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
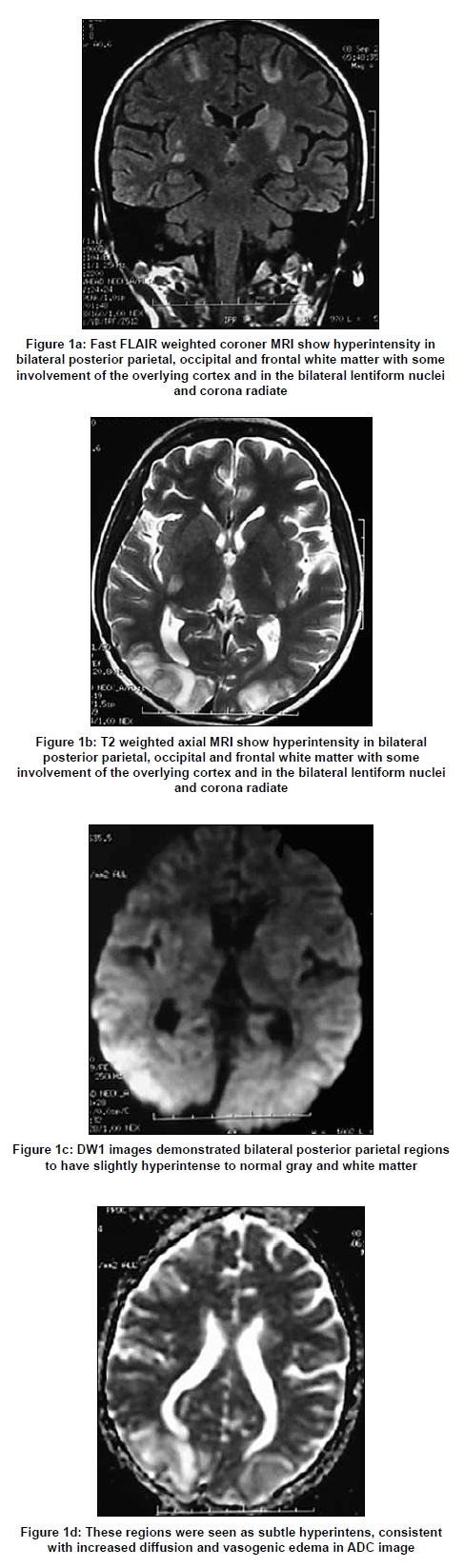
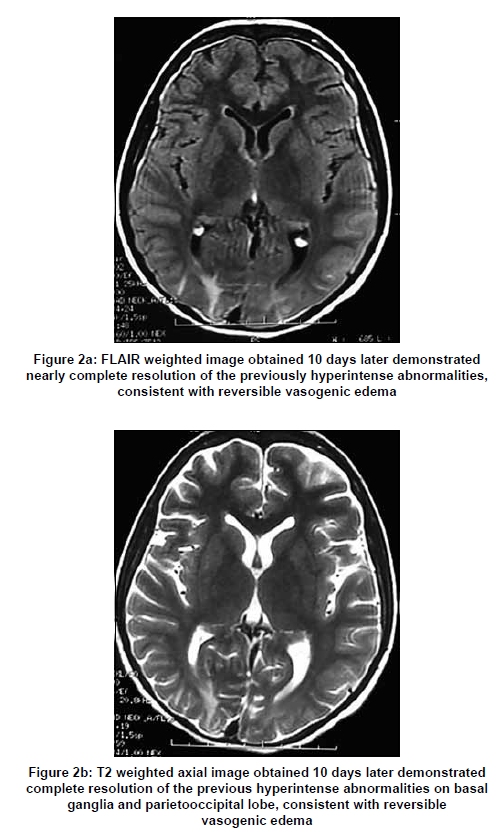
Neurology India, Vol. 57, No. 4, July-August, 2009, pp. 497-499 Letter To Editor Posterior reversible encephalopathy syndrome in systemic lupus erythematosus Necioglu Orken Dilek, Kenangil Gulay, Ur Emel, H. Forta Department of Neurology, Sisli Etfal Education and Research Hospital, Istanbul Correspondence Address: Department of Neurology, Sisli Etfal Education and Research Hospital, Istanbul, dilek.necioglu@gmail.com Date of Acceptance: 02-Jul-2009 Code Number: ni09139 PMID: 19770558 DOI: 10.4103/0028-3886.55571 Sir, Posterior reversible encephalopathy syndrome (PRES) is a rapidly resolving neurological condition characterized by headache, nausea, vomiting, altered mental status, visual disturbances, and seizures. [1] It is associated with a multitude of diverse clinical entities. [1] A case of PRES in a systemic lupus erythematosus (SLE) patient is reported here due to its rarity. A 22-year-old female, diagnosed with SLE at age 19 after presenting with arthritis and nephritis, a positive antinuclear antibody and elevated double-standed (ds) DNA, was admitted to the hospital with an acute deep venous thrombosis (DVT). She was treated with Enoxaparine sodium 60mg bid. During the hospitalization, she had an episode of acute arthralgia accompanied by hypoalbuminemia, acitis and generalized edema and treated with intravenous pulse dose metilprednisolone, one dose cyclophosphamide and furosemide infusion. On 10 th day, she experienced generalized tonic-clonic seizure, which was controlled by the administration of intravenous diazepam and subsequent loading dose of phenytoin sodium. Her blood pressure was 155/115mmHg. She was alert, with normal mental status. She had blurring of vision and bilateral extensor plantar responses without any motor deficit. A noncontrast cranial computed tomography (CT) demonstrated multiple focal areas of hypodensity bilaterally in the basal ganglia, parietal, and occipital lobes. The differential diagnosis at this point included central venous thrombosis (CVT), multiple embolic lesions, vertebrobasilar thromboocclusive disease, or widespread inflammatory disease secondary to lupus involving the central nervous system (CNS). Lumbar puncture demonstrated opening pressure of 180cm H 2 O with normal cell counts, protein, and glucose levels. Subsequent magnetic resonance imaging (MRI) of the brain confirmed high signal intensity on axial T2 and fluid-attenuated inversion recovery (FLAIR) weighted images in those regions explained on CT and additionally on both frontal lobes. Diffusion-weighted (DW1) images and apparent diffusion coefficient (ADC) map showed slightly hyperintense lesions, compared to normal gray and white matter, consistent with vasogenic edema [Figure - 1]. Cranial magnetic resonance venography was normal. The patient was diagnosed as PRES. The abnormalities of vision improved after 48 hours and resolved within five days. The blood pressure was controlled. Ten days after the insult, repeated MRI demonstrated nearly complete resolution of the previously hyperintense lesions. The size of the lesions in right occipital and frontal regions got smaller but persisted [Figure - 2]. The abrupt onset of CNS symptoms in SLE patients presents a diagnostic and therapeutic challenge. As reported on a recent review of 323 SLE patients, the most common CNS presentations in descending order of frequency were headache, cerebrovascular disease, mood disorders, cognitive dysfunction, seizures, psychosis, anxiety disorder, and acute confusional state.[2] These symptoms may be either due to direct immune mediated injury of the CNS or secondary events (i.e., related to complication of SLE or its treatment). PRES is an acute or subacute, progressive reversible neurologic syndrome which can mimic neuropsychiatric SLE presentations. Hence, in SLE patients with acute neurologic symptoms in the setting of hypertension, renal insufficiency and immunosuppressive treatment, PRES should be considered as the cause of CNS abnormalities.[3] A total of 30 cases of PRES in SLE patients have been reported in the literature but the true prevalence is unclear. [4] In recent years, another MR technique, echo- planar DWI findings are useful in distinguishing PRES from neuropsychiatric SLE presentations. Regions with vasogenic edema show marked hyperintensity on ADC and mostly iso or hypointensity on DWI. [5] Although the lesions of our patients challenge with this knowledge, according to Ay et al . an increase in T2 signal within regions of vasogenic edema (T2 shine-through) could cause slight DW1 hyperintensity. [5] In conclusion, PRES should be recognized in patients with SLE presenting with CNS findings. It is extremely important to distinguish this syndrome from other causes, since it is reversible and readily treated by controlling blood pressure, discontinuing the offending immunosuppressive agent or decreasing the dose and controlling of seizure activity. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09139f2.jpg] [ni09139f1.jpg] |
| |||||||||

{kind=link}
{kind=link}