 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
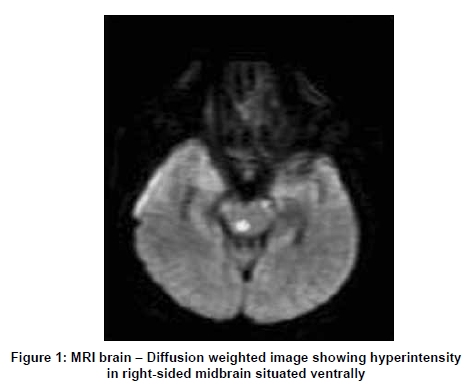
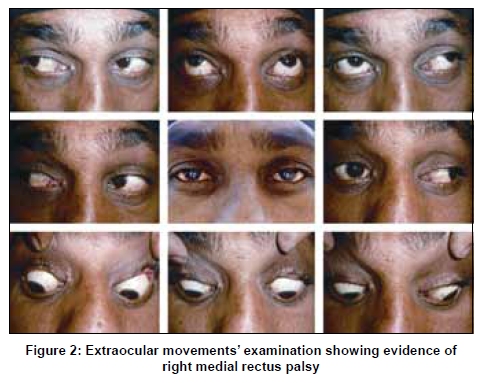
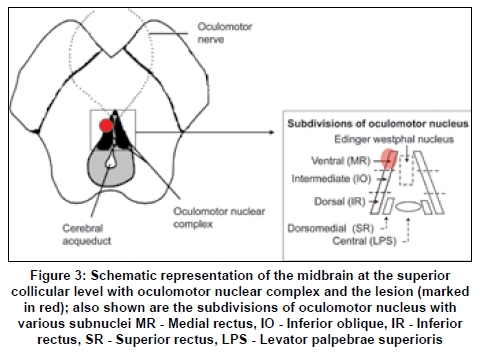
Neurology India, Vol. 57, No. 4, July-August, 2009, pp. 499-501 Letter To Editor Midbrain infarct presenting as isolated medial rectus palsy Simerpreet Bal, Vivek Lal, Dheeraj Khurana, Sudesh Prabhakar Department of Neurology, Postgraduate Institute of Medical Education and Research, Chandigarh - 160 012, India Correspondence Address: Department of Neurology, Postgraduate Institute of Medical Education and Research, Chandigarh - 160 012, vivekl44@yahoo.com Date of Acceptance: 26-Feb-2009 Code Number: ni09140 PMID: 19770560 DOI: 10.4103/0028-3886.55579 Sir, A 30-year-old man, labourer by occupation, presented with sudden onset of giddiness followed by diplopia with horizontal separation of images on looking to extreme left gaze. On examination, hemodynamics were normal and neurological examination showed right medial rectus palsy [Figure - 1]. Magnetic resonance imaging (MRI) of the brain showed a hyperintensity in rostral midbrain in diffusion weighted images [Figure - 2] and flair images. He was thoroughly investigated for the causes of young stroke and was found to have dyslipidemia, which was treated with cholesterol-lowering agents and antiplatelets. The patient received visual tracking eye exercises during his hospital stay and his complaints resolved within three weeks. Oculomotor nerve has two motor nuclei, the main motor nucleus and the accessory parasymphathetic nucleus. The main oculomotor nucleus which is situated in the anterior part of the gray matter surrounding the cerebral acqueduct of the midbrain at the level of superior colliculus supplies all the extrinsic muscles of the eye except the superior oblique and lateral rectus muscle. It consists of one unpaired central caudal nucleus for bilateral levator palpebrae superioris and four paired subnuclei. [1] The subnucleus for superior rectus muscle is situated dorsomedially and decussation of the fibers to the superior rectus takes place within the oculomotor nuclear complex; thus, lesions affecting the nucleus may simultaneously involve ipsilater al superior rectus subnuclei as well as crossing fibers resulting in bilateral superior rectus muscle palsy. [2] Ventral to the superior rectus subnuclei lies the subnuclei for ipsilateral inferior rectus followed by intermediate subnuclei for ipsilateral inferior oblique and the most ventrally situated subnuclei is for ipsilateral medial rectus [Figure - 3]. Third nerve nuclear lesions cause weakness of bilateral superior rectus muscle ipsilateral inferior oblique, inferior rectus, medial rectus, with bilateral partial ptosis (due to involvement of central caudal subnuclei supplying both levator palpebrae superioris). This is a case of nuclear oculomotor nerve palsy with an unusual presentation due to strategic location of infarct in the rostral midbrain involving the medial rectus subnuclei which is situated most ventrally and can be diagnosed with diffusion weighted imaging (DWI). [3] Unilateral ocular palsy is commonly seen with lesions in the orbit or from muscular diseases and rarely from a third nerve nuclear lesion, though inferior oblique muscle palsy caused by involvement of intermediate subnuclei [4] and isolated inferior rectus palsy due to ipsilateral involvement of dorsally situated subnuclei or fascicular lesions have been described. [5] With use of DWI and other multimodality MRI the probability of picking up midbrain infarcts causing isolated oculomotor palsies have increased. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09140f1.jpg] [ni09140f3.jpg] [ni09140f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}