 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
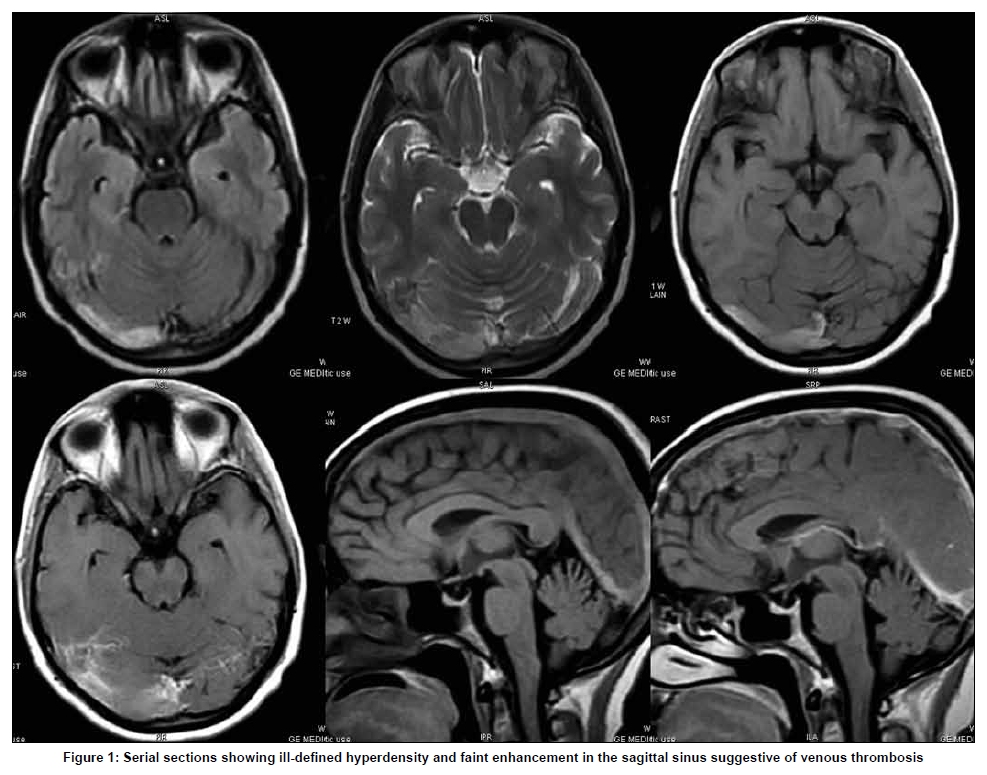
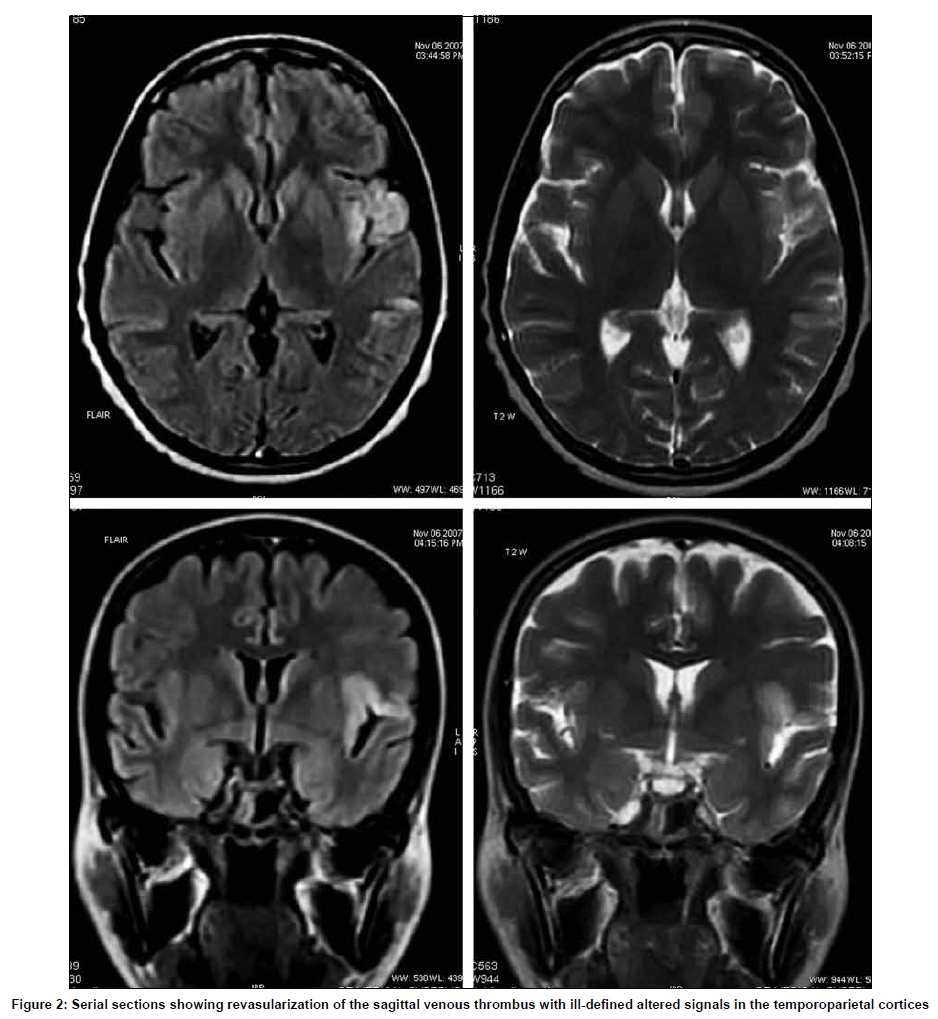
Neurology India, Vol. 57, No. 4, July-August, 2009, pp. 505-507 Letter To Editor Choriocarcinoma with arterial and venous thrombosis Sanju Cyriac, T. G. Sagar, Vandana Mahajan Cancer Institute (WIA), Chennai, India Correspondence Address: Cancer Institute (WIA), Chennai, India, drsanpan80@yahoo.com Date of Acceptance: 18-Feb-2009 Code Number: ni09144 PMID: 19770564 DOI: 10.4103/0028-3886.55586 Sir, The treatment of choriocarcinoma forms one of the success stories of oncology with survival rates of nearly 100% in low-risk group and more than 90% in the high-risk group. [1] It is a unique neoplasm with a great propensity for spread by hematogenous route, including to the brain. The central nervous system (CNS) metastasis is often hemorrhagic and thormbotic complications are extremely rare. A 30-year-old lady presented with bleeding per vaginum of two months duration. The obstetric history revealed a normal delivery five years back, a spontaneous abortion four years back, and a molar pregnancy two years back for which evacuation was done. Serum human chorionic gonadotropin (HCG) was 90000IU. Computerized tomography (CT) of the chest revealed multiple bilateral lung metastasis. CT of the brain was normal. Based on the history and high HCG values, she was diagnosed to have choriocarcinoma, stage III high risk (WHO score 8), and was initiated on etoposide, methotrexate, actinomycin-D, cyclophosphamide, and vincristine (EMACO) chemotherapy. She responded to treatment with dropping HCG values. After two cycles of the therapy, she had an episode of generalized tonic-clonic seizures. Magnetic resonance imaging (MRI) was suggestive of cerebral venous thrombosis [Figure - 1]. Enoxaparin treatment was initiated and was later continued on warfarin. Once her general condition improved EMACO was reinitiated. After two more cycles of the therapy, she had sudden onset right-sided hemiparesis and MRI brain this time was suggestive of left temporal lobe infarct with edema [Figure - 2]. Coagulation screening including serum antiphospholipid antibody was normal. Echocardiogram did not reveal any vegetations or septal defects. She was continued on anticoagulants which was stopped only after HCG normalized. The patient received six cycles of chemotherapy, her HCG values normalized and now she has completed 15 months of follow up. She is in remission and does not have any residual neurological deficits. Gestation trophoblastic neoplasia represents one of the success stories of modern-era chemotherapy in the treatment of human malignancy. The incidence of choriocarcinoma varies from 1 in 120 pregnancies in some parts of Asia to 1 in 1200 in United States.[1] Choriocarcinoma has the propensity for vascular invasion and widespread metastasis, including to the brain. CNS metastasis is usually hemorrhagic and our patient had normal study of brain upfront and developed the neurological events while on treatment. CNS in volvement in Choriocarcinoma can be due to hemorrhagic metastas, tumor embolization and chemotherapy (especially platinum compounds). CNS thrombotic events are extremely rare. The association between cancer and thrombosis was identified in 1865 and the combination is called as Trousseau syndrome. [2] The mechanisms elucidated include cytokines like TNFa, IL-1, and IL-6 that cause endothelial damage resulting in thrombosis. [3] The interaction between tumor cells and macrophages activates platelets and factors XII and X, which leads to thrombin generation and thrombosis. The various chemotherapeutic agents including platinum compounds can cause endothelial damage. Central venous catheters and total parenteral nutrition also increase the risk. Lepidini et al . reported a patient with pure testicular choriocarcinoma who suffered from both arterial and venous thrombosis during chemotherapy. [4] An increased paraneoplastic stimulus of HCG, secondary to the marker surge phenomenon, was suggested as responsible for transient hypercoagulability and subsequent thromboembolism. Komeichi et al . had an interesting case of metastatic choriocarcinoma associated with cerebral thrombosis and aneurysmal formation. [5] The aneurysmal wall was invaded by choriocarcinoma. To the best of our knowledge, this is the first reported case of choriocarcinoma with cerebral venous thrombosis during the course of the treatment. Cerebral thrombotic events also should be borne in mind, when a patient with choriocarcinoma presents with focal deficits. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09144f1.jpg] [ni09144f2.jpg] |
| |||||||||

{kind=link}
{kind=link}