 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
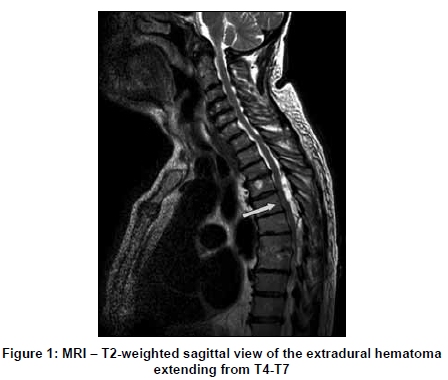
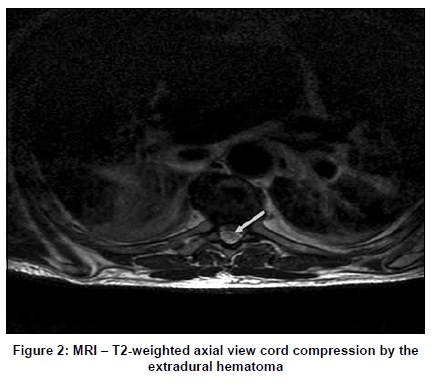
Neurology India, Vol. 57, No. 4, July-August, 2009, pp. 512-513 Letter To Editor Spinal epidural hematoma after insertion of a thoracic epidural catheter in the absence of coagulation disorders - A call for raised awareness Bahram Fakouri, Shreya Srinivas, Sani Magaji, Alex Kunsky, Francesco Cacciola Queen's Medical Centre, Centre for Spinal Studies and Surgery, Nottingham, United Kingdom Correspondence Address: Queen's Medical Centre, Centre for Spinal Studies and Surgery, Nottingham, United Kingdom, rancesco.cacciola@gmail.com Date of Acceptance: 31-Mar-2009 Code Number: ni09148 PMID: 19770568 DOI: 10.4103/0028-3886.55590 Sir, Thoracic epidural catheterization for postoperative analgesia is relatively a safe procedure with an extremely low incidence of neurological complications and the reported maximum risk was 0.07%. [1] Of the 4000 patient records analyzed in this study, no instance of spinal epidural hematoma (SEH) was encountered. There have been case reports of epidural hematoma seen 'after removal' of an epidural catheter. This complication is also exceptional and the estimated frequency was 1 out of 150,000 to 190,000 procedures. [2] In most of these cases, risk factors such as coagulopathy or anticoagulation treatment were present. In a patient who has undergone major surgery and does not have any risk factors like coagulation disorders or traumatic catheter insertions, a SEH is thus generally unexpected and could easily be diagnosed too late. A 74-year-old male had undergone a major abdominal surgery under thoracic spinal epidural anesthesia. Thoracic edpidual catheter placement was uneventful and there was no trauma. The patient did not have any preoperative coagulopathy. A good analgesic regime through the catheter guaranteed the absence of any pain during intraoperative period and for a couple of hours postoperatively the patient did not wake up. It was only around five hours postoperatively, when he was alert a vigorous stimulus failed to evoke any pain or motor response in the lower limbs. This alerted the clinicians the suspicion of a complication. Neurological examination revealed complete paraplegia involving both pyramidal and all the sensory tracts. Magnetic resonance imaging (MRI) showed a large SEH extending from T4 to T7 causing massive cord compression [Figure - 1] and [Figure - 2]. Around 10 hours post catheter insertion surgical decompression was done. He regained the ability to walk with crutches. This case illustrates the necessity to treat SEH as an absolute emergency. The earlier one operates, preferably within 12 hours, the better will be the outcomes. [3] Pain, the most common presenting symptom of SEH, is usually absent in cases of epidural catheter analgesia related SEH. Thus in the given clinical setting, awareness and early diagnosis of SEH is of paramount importance to achieve good surgical outcomes. Patient cooperation in the clinical evaluation is also important. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09148f1.jpg] [ni09148f2.jpg] |
| |||||||||

{kind=link}
{kind=link}