 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
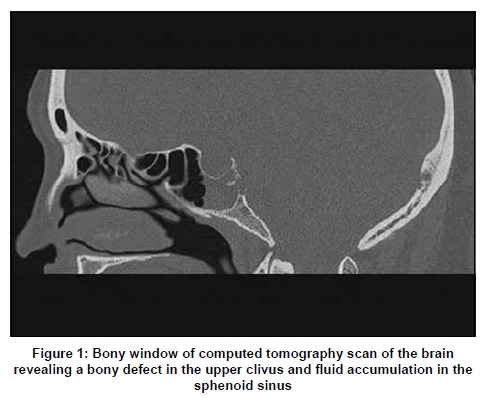
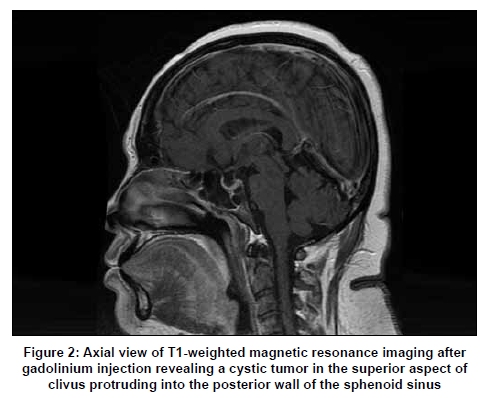
Neurology India, Vol. 57, No. 4, July-August, 2009, pp. 513-514 Letter To Editor Spontaneous cerebrospinal fluid rhinorrhea: A rare initial presentation of clival chordoma Cheng-Ta Hsieh, Ming-Ying Liu, Wan-Fu Su1, Da-Tong Ju Departments of Neurological Surgery, 1Otolaryngology-Head and Neck Surgery, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan, Republic of China. Correspondence Address: Department of Neurological Surgery, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan, Republic of China, nogor@mail2000.com.tw Date of Acceptance: 21-Mar-2009 Code Number: ni09149 PMID: 19770569 DOI: 10.4103/0028-3886.55591 Sir, Chordoma is a rare bony tumor that accounts for approximately 1% of intracranial tumors. [1] Headache and progressive cranial nerve palsies are characteristic presenting features of clival chordoma. [2] Spontaneous cerebrospinal fluid (CSF) rhinorrhea as the initial manifestation of clival chordoma is extremely rare. [1] A 47-year-old female was admitted for clear nasal discharge and intermittent headache of five months duration. Prone or head-down position with valsalva maneuver would lead to significant rhinorrhea. She denied any history of head trauma. Neurological examination was unremarkable. Computed tomography (CT) showed an osteolytic mass with cystic component in the clivus [Figure - 1]. Magnetic resonance imaging (MRI) of the brain showed a cystic tumor measuring about 1cm in diameter with fleck of calcification in the superior aspect of clivus. The mass was protruding into the posterior wall of the sphenoid sinus with destruction of adjacent dura resulting in a fistulous tract between the prepontine CSF space and sphenoid sinus [Figure - 2]. She underwent endonasal trans-sphenoidal surgery for removal of the tumor and repair of the leakage. At operation, there was descent of the sella diaphragm and CSF leak was seen coming from the bony defect invaded by the tumor. The tumor origin was from upper part of the clivus. After removal of the tumor, the bony defect was packed with adipose tissue harvested from lower abdomen and fibrin glue. Pathological examinations of the excised lesion confirmed the diagnosis of chordoma. Postoperatively, she had relief of headache and there was no more CSF rhinnorhea. Chordoma, a tumor arising from notochordal remnants, is a rare bony lesion, with a reported incidence of 0.2-0.5 per 100,000 population. [3],[4] It accounts for less than 0.5% of all skull-base tumors. [1] Of all the chordomas, skull-base chordomas account for 35%. [2] Clival chordoma is most common in the third and further decades and affects either gender equally. Although chordoma is a slow-growing benign tumor, it can rarely metastasize. It is considered clinically malignant because of the recurrence and invasive nature. [4] Because of the location, skull-base chordomas often present with headaches and diplopia and sixth and fifth nerve palsies are the most common neurological signs. [1],[2] The interval between onset of symptoms and diagnosis of clival chordoma is quite variable, 2.5-4.4 years. [4] The uncommon clinical presentations include: Nasal obstruction, nasal bleeding, and subarachnoid hemorrhage. [3],[5] Spontaneous CSF rhinorrhea without neurological deficits as the initially manifestation of clival chordoma has rarely been reported. In one report of 14 patients with clival chordomas, two patients presented with spontaneous CSF rhinorrhea.[1] However, in this report the authors had not detailed the clinical characteristics of the two patients. In cases of spontaneous CSF leak, high-resolution CT scanning is the best investigative modality to evaluate the detail of bony structures of parasinus walls and skull base. MRI is helpful to investigate the soft tissue and possible site of leak. With the advance of microscopic and endoscopic techniques, endonasal trans-sphenoidal method is the best method to prove the diagnosis and also to repair the leak. [1] References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09149f1.jpg] [ni09149f2.jpg] |
| |||||||||

{kind=link}
{kind=link}