 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
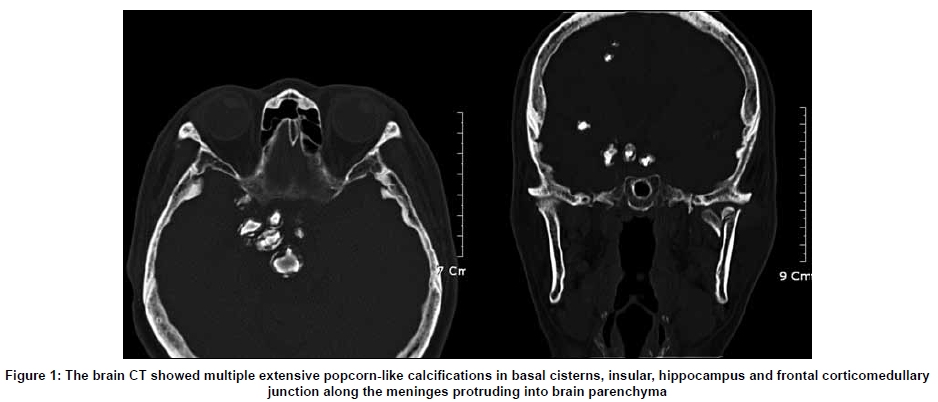
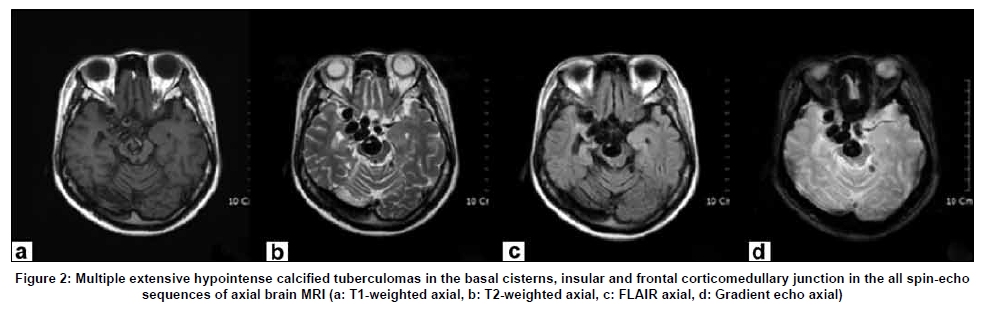
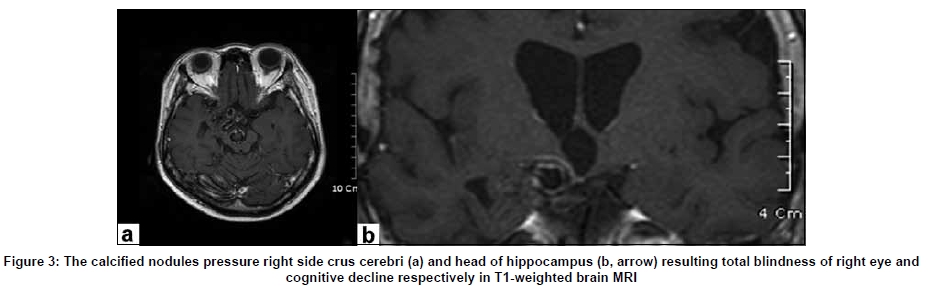
Neurology India, Vol. 57, No. 4, July-August, 2009, pp. 521-522 Neuroimage Extensive meningeal and prenchymal calcified tuberculoma as long-term residual sequelae of tuberculous meningitis Bon D. Ku, Seung Don Yoo1 Department of Neurology, Myongji Hospital, 697-24, Hwajung-dong Dukyang-gu Goyang, South Korea, Correspondence Address: Prof. Bon D. Ku, Department of Neurology, Myongji Hospital, 697-24, Hwajung-dong Dukyang-gu Goyang, South Korea. neurodasan@paran.com Date of Acceptance: 09-Feb-2009 Code Number: ni09158 PMID: 19770574 DOI: 10.4103/0028-3886.55593 A 51-year-old woman presented with progressive cognitive decline of 1 year duration. Her past medical history revealed that she received treatment for tuberculous meningitis and milliary tuberculosis at the age of twenty. At that time cerebrospinal fluid (CSF) and sputum were positive for M. tuberculosis . During that illness she had suffered from recurrent seizures. Neurological examination revealed right optic atrophy with total blindness and right spastic hemiparesis. Neuropsychological tests revealed visuospatial, verbal and visual memory deficits, and also deficits in frontal executive functions. Brain computed tomography (CT) scan and magnetic resonance imaging (MRI) showed multiple extensive popcorn-like calcifications in the basal cisterns, insula, hippocampus, and frontal corticomedullary junction along the meninges protruding into the brain prenchyma [Figure - 1] and [Figure - 2]. The masses showed hypointensity in all spin-echo sequences of the brain MRI [Figure - 2]. These findings suggest extensive meningeal and parenchymal calcified tuberculoma as long-term sequelae of tuberculous meningitis. A large calcified nodule in the right crus cerebri was probably responsible for the blindness in her right eye and a right hippocampal head compression by the calcified lesion may relate to some of her cognitive deficits [Figure - 3]. Tuberculosis usually involves the brain through hematogenous spread. Hematogenously disseminated M. tuberculosis lodge in the corticomedullary junctions where a rupture into the subarachnoid space leads to meningeal infection and granuloma formation in the base cisterns. [1] These focal granulomas may go through calcific stage. [1],[2] Calcified tuberculomas as a sequelae of meningitis usually appear markedly hypointense on all spin-echo sequences. [2] An isointense or hypointense core with a hyperintense rim on T2-weighted and fluid attenuated inversion recovery (FLAIR) images is the most common presentation.[2] The inhomogeneous ring-like high signal in the T1-weighted image suggests peripheral gliotic changes of calcification. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09158f2.jpg] [ni09158f3.jpg] [ni09158f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}