 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
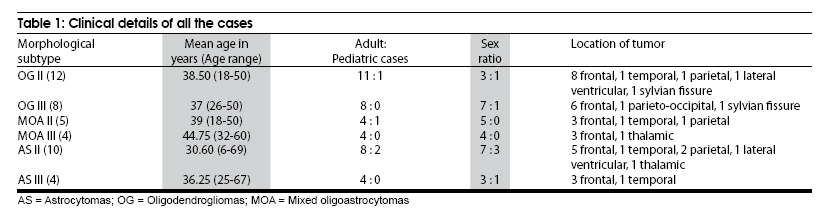
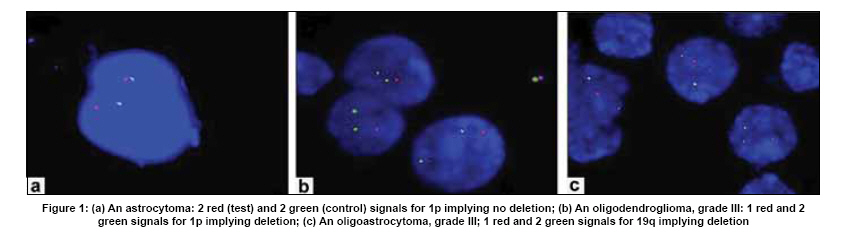
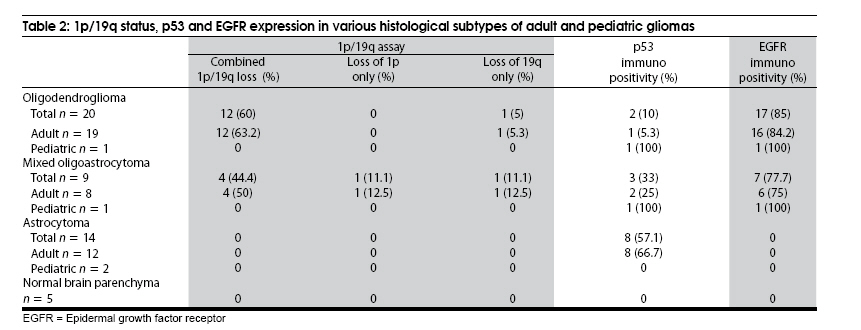
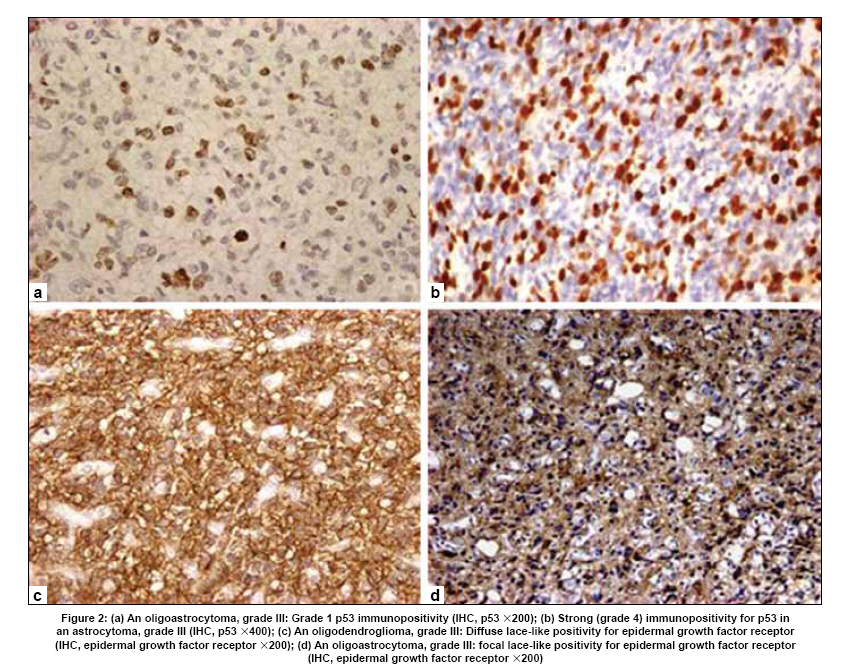
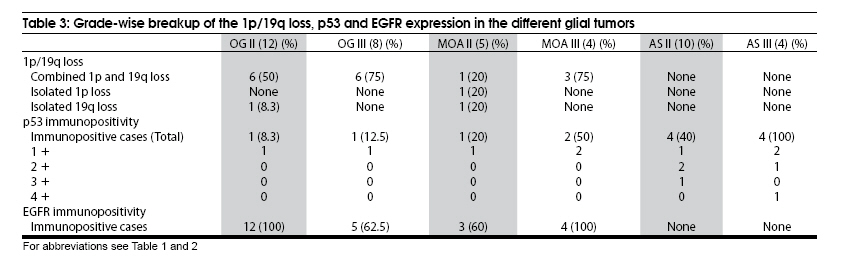
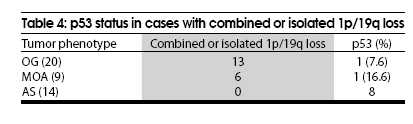
Neurology India, Vol. 57, No. 5, September-October, 2009, pp. 559-566 Original Article Assessment of 1p/19q status by fluorescence in situ hybridization assay: A comparative study in oligodendroglial, mixed oligoastrocytic and astrocytic tumors Bhaskar Shukla, Shipra Agarwal, Vaishali Suri, Pankaj Pathak, Mehar Chand Sharma, Deepak Gupta1 , Bhavani Shankar Sharma1 , Ashish Suri 1 , Ashutosh Halder 2 , Chitra Sarkar Departments of Pathology, 1 Neurosurgery, and 2 Reproductive Biology, All India Institute of Medical Sciences, New Delhi, India Date of Acceptance: 09-Oct-2009 Code Number: ni09164 PMID: 19934553 DOI: 10.4103/0028-3886.57795 Abstract Background : Due to overlapping histomorphological features, difference in clinical behavior and treatment response, establishing potential molecular markers to facilitate diagnosis of various genetic subtypes of diffuse gliomas is essential.Aim : To analyze 1p/19q status in diffuse gliomas and correlate it with epidermal growth factor receptor (EGFR) and p53 protein expression. Materials and Methods : 1p/19q status in 43 cases was evaluated by fluorescence in situ hybridization assay. Glial fibrillary acidic protein (GFAP), EGFR and p53 were assessed by immunohistochemistry. Results : Glial fibrillary acidic protein immunopositivity was observed in oligodendrogliomas within minigemistocytes and gliofibrillary oligodendrocytes as perinuclear homogenous blobs. It also highlighted the intermingled reactive astrocytes. Astrocytomas and the astrocytic component of oligoastrocytomas showed a diffuse fibrillary type of staining. 1p and/or 19q loss was seen in 65% (13/20) of oligodendrogliomas and 66.6% (5/9) of mixed oligoastrocytomas. There was one case each of pediatric oligodendroglioma and mixed oligoastrocytoma, none of which showed 1p/19q loss. None of the astrocytomas including two pediatric cases showed this alteration (P < 0.05). p53 was expressed in 57.1% of astrocytomas (8/14), 33% of mixed oligoastrocytomas (3/9) and 10% of oligodendrogliomas (2/20). Majority of oligodendrogliomas (85%; 17/20) and oligodendroglial areas in mixed oligoastrocytomas (77.7%; 7/9) showed a membranous lace-like immunopositivity with EGFR. In contrast, all astrocytomas (Grade II and III) were EGFR negative. Conclusion : Loss of 1p/19q is strongly associated with oligodendroglial phenotype, while astrocytic tumors are more likely to show p53 over-expression. p53 expression and 1p/19q status appear to be mutually exclusive. Keywords: Fluorescence in situ hybridization, glioma, p53 protein, 1p/19q Introduction Incidence of gliomas is around 5-10 per 100 000 in the general population making them the most common primary brain tumors in adults. [1] World Health Organization (WHO) classifies gliomas into astrocytomas (AS), oligodendrogliomas (OG) and mixed oligoastrocytomas (MOA). [2] Over the past 20 years a number of chromosomal, genetic and epigenetic alterations have been found to be associated with different histological types and malignancy grades of gliomas. In this direction, OGs represent the first central nervous system (CNS) neoplasms in which a genetic signature has been correlated with improved outcome. In 1994, Reifenberger et al., demonstrated allelic loss of chromosome 19q in 81% of the oligodendroglial tumors. Of these, approximately 75% also exhibited loss of heterozygosity (LOH) at 1p locus. [3] Subsequently several studies confirmed that combined loss of large chromosomal regions at these loci is a hallmark of oligodendendroglial tumors. [4] In addition, these genetic alterations have been linked to the clinical outcome. The allelic loss of chromosome 1p has been found to be a statistically significant predictor of chemosensitivity, and combined LOH of 1p/19q to be associated not only with chemosensitivity, but also with a longer recurrence-free survival after chemotherapy. [5],[6],[7] The incidence of p53 gene mutations is not as frequent in OGs as it is in ASs, remaining within the range of 10-20%, [8],[9] and is more common in OGs with an intact 1p or 19q. [10] Another molecular marker that has been variably studied in gliomas is epidermal growth factor receptor (EGFR). Though EGFR overexpression is reportedly common in OGs, [11],[12] amplification of its gene is rare in these neoplasms. [13] This study was undertaken to assess the molecular profile of OGs and MOAs (grade II and III) in terms of 1p/19q status, p53 and EGFR expression, and compare it with ASs of corresponding grade. To the best of our knowledge, this is the first report on fluorescence in situ hybridization (FISH) analysis of a representative cohort of gliomas from India. Materials and Methods Clinical data Neuropathology records of the All India Institute of Medical Sciences, New Delhi, India between January 2007 and December 2007 were reviewed. Of the 384 cases of glioma seen during the study period, 74% of the tumors were ASs, and oligodendroglial differentiation was seen in 52 cases. Demographic data, age and sex of the patients were noted. Histopathological examination Of the 52 cases with oligodendroglial differentiation, 29 (20 OG and 9 MOA) cases where enough material was available in the paraffin blocks, were selected for further analysis. Fourteen age and sex-matched cases of AS were also included. The original hematoxylin and eosin (H and E) slides were re-evaluated independently by four neuropathologists (CS, VS, BS and SA). The diagnosis was reconfirmed as per the recent WHO classification. [2] Age and sex-matched normal cortical brain tissue from epilepsy surgery cases was chosen as control. Immunohistochemical staining for glial fibrillary acidic protein, p53 and epidermal growth factor receptor Monoclonal antibodies for glial fibrillary acidic protein (GFAP) (Dako Denmark, dilution, 1:1000), p53-DO1 (Santa Cruz, Biotechnology, Inc. dilution, 1:200) and EGFR-NCL (Dako Denmark, dilution, 1:50) were used. Labeled streptavidin biotin kit (Universal) was used as detection system (Dako, Denmark). For GFAP, antigen retrieval was not required. For EGFR immunostaining, protease digestion (DAKO S 3020) was performed. Antigen retrieval for p53 staining was done using 0.01 M citrate buffer, pH 6.0. For p53, cases where more than 10% of nuclei showed positivity were considered as positive. Immunopositive cases were graded from 1 + to 4 + as follows: 1 + positivity: 11-25% cells stained; 2 + positivity: 26-50% cells stained; 3 + positivity: 51-75% cells stained and 4 + positivity: 76-100% cells stained. Fluorescence in situ hybridization analysis of 1p and 19q In all the selected cases, dual-probe FISH assay was performed on paraffin-embedded sections, with locus-specific probes for 1p36 and 19q13 paired, respectively, with the reference probes for 1q25 and 19p13 (Vysis, Downers Grove, IL). Target retrieval was achieved using citrate buffer, pH 6.0 and boiling in microwave for 20 min. Slides were exposed to 0.04% pepsin (P-7000; Sigma- Aldrich, St. Louis, MO) digestion for 30 min at 37°C. Probe mixture (10 μL per slide) was applied. Simultaneous probe/specimen denaturation at 73°C for 5 min with subsequent overnight incubation at 37°C was performed in Thermobrite TM hybridization chamber (Vysis Inc). The sections were washed the next day in 2X SSC (2 min at 73°C) followed by 0.5X SSC (2 min at room temp) and counterstained with 4, 6-diamidino-2-phenylindole (Vysis) and visualized under a fluorescence microscope. Signals were scored in at least 200 non-overlapping, intact nuclei. At least 50% or more nuclei had to show one signal to be scored as a deletion. [14] Statistical analysis Descriptive statistics i.e. mean and frequency distribution was calculated for all the variables. According to the different categories for the categorized variables, Chi-square test and Fisher's exact test were applied. A P-value of 0.05 was considered as statistical significance level. SPSS statistical software was used for the statistical analysis. Results Three hundred and eighty-four glial tumors were received in the Department of Pathology between January 2007 and December 2007. Of these, a large majority (74%) were ASs, followed by ependymomas (12.5%). The pure OGs and MOAs comprised 10.4% (40) and 3.1% (12) of all these cases. All were tumor excision specimens. Of the 20 cases of pure OG included in the study, 12 (60%) were grade II and 8 (40%) grade III. Of the 9 MOAs, 5 (55.6%) were grade II, 4 (44.4%) grade III; and amongst the 14 ASs (36.95%), 10 (71.4%) were grade II and 4 (28.6%) grade III. Thirty-nine tumors occurred in adults (more than 18 years of age). There were 4 pediatric cases, 2 AS Grade II, 1 OG grade II and 1 MOA grade II. Male preponderance was seen in all the histological types. Most of the tumors were frontal in location followed by temporal [Table - 1]. Rest involved other sites such as parietal lobe, sylvian fissure, intraventricular and thalamic. Histological features Oligodendrogliomas Oligodendrogliomas grade II were characterized by a diffuse infiltrate of monomorphic cells with uniform round nuclei and perinuclear halo artifact giving rise to the so-called honeycomb pattern. There was a dense network of branching capillaries in all the cases along with foci of microcalcifications. Minigemistocytes, as identified by the presence of perinuclear eosinophilic cytoplasm and the halo between this cytoplasm and the cell membrane, were also identified interspersed in between the tumor cells. Gliofibrillary oligodendrocytes were morphologically similar to classical oligodendroglial cell and had thin perinuclear wispy cytoplasm. Oligodendrogliomas grade III were characterized by the presence of increased mitotic activity, microvascular proliferation and foci of necrosis. Oligoastrocytomas Within MOAs, the oligodendroglial and astrocytic component was either diffusely intermingled or separated into distinct (biphasic) areas. Mixed oligoastrocytomas grade III were characterized by features of anaplasia, including cellular pleomorphism, nuclear atypia, high cellularity, prominent mitotic activity, microvascular proliferation and foci of necrosis. Astrocytomas All cases of diffuse ASs (grade II) were characterized by well-differentiated fibrillary neoplastic astrocytes, with moderately increased cellularity and occasional nuclear atypia. Two of these cases, in addition, showed focal areas of gemistocytic neoplastic astrocytes. Anaplastic ASs in contrast, had a higher cellularity, distinct nuclear atypia and prominent mitotic activity. Microvascular proliferation and necrosis were absent in all the cases. Glial fibrillary acidic protein expression Glial fibrillary acidic protein stained the minigemistocytes and gliofibrillary oligodendrocytes, at least focally, in all cases of OGs grade II, in the form of a perinuclear homogenous blob. Scattered reactive astrocytes were also highlighted. Only occasional cells in cases of OGs grade III showed the perinuclear positivity with GFAP. It also stained the fibrillary processes of the tumor cells in all AS cases. The oligodendroglial and astroglial components in the cases of MOAs grade II showed the same immunoreactivity patterns as in cases of pure OG and AS, respectively. However, immunostaining was focal in the oligodendroglial areas of MOAs grade III. Fluorescence in situ hybridization assay Majority (60%) of OGs harbored combined 1p/19q loss (12/20) [Figure - 1]. These included 50% of grade II (6/12) and 75% of grade III OGs (6/8). Isolated 19q deletion was seen in 5% of OGs (1/20), which on histomorphology belonged to WHO grade II. Lone 1p loss was not found in any of the OGs. Amongst the MOAs, combined 1p/19q loss was observed in 44.4% cases (4/9), including one grade II and 3 grade III tumors. Approximately 11.1% showed isolated 1p loss (1/9). A similar percentage showed lone 19q loss [Figure - 1]. Both these were grade II tumors. None of the grade III MOAs harbored isolated chromosomal abnormalities. However, interestingly, none of the two pediatric cases with oligodendroglial differentiation showed 1p/19q loss [Table - 2]. In contrast to OGs and MOAs, none of the ASs showed loss of 1p and/or 19q [Figure - 1]. None of the five control cases showed either combined or isolated 1p/19q loss [Table - 2]. On statistical analysis, the oligodendroglial phenotype was found to be significantly associated with a loss of 1p ( P < 0.05), a loss of 19q ( P < 0.05) and a combined loss of 1p and 19q (P < 0.05). p53 expression p53 immunopositivity was very rare in oligoden drogliomas. Only 10% cases were p53 immunopositive (1 grade II and 1 grade III OG). In MOAs, p53 immunopositivity was observed in 33% cases (3/9) [Figure - 2]. Majority (8/14; 57.1%) of the ASs showed p53 protein expression [Figure - 2]. Interestingly, the intensity of staining was weak (grade 1) in the p53-immunopositive OGs and MOAs. In contrast, majority (70%) of the p53-immunopositive ASs showed good-to-intense (grade 2-4) staining [Table - 3]. Therefore OGs are less likely to show p53 protein overexpression as compared to ASs and this was statistically significant (P = 0.018). Also, p53 expression was higher in grade III tumors when compared with grade II tumors [Table - 3]. Majority of the cases, which showed either combined or isolated loss of 1p/19q, did not show p53 expression. Only 1 case of OG and 1 MOA carrying this molecular alteration showed concomitant p53 immunopositivity [Table - 4]. However, the intensity of staining in these two cases was weak (grade 1). Thus, 1p and/or 19q deletion and p53 protein expression appear to be mutually exclusive events. Epidermal growth factor receptor expression A peculiar diffuse lace-like pattern of immunopositivity was observed in majority of OGs (85%; 17/20) and MOAs (77.7%; 7/9) [Figure - 2]. It was helpful in identifying even a small focus of oligodendroglioma in MOAs. All the AS (grades II and III) and the astrocytic component of MOAs were EGFR negative. Discussion Gliomas are the most common primary brain tumors in adults. [15] Their pathological evaluation and subtyping relies mainly on the light microscopic appearance. Although the histomorphologic criteria for their diagnoses are well established, a significant proportion of cases pose diagnostic challenge. Difficulties in clinical behavior and response to therapy warrant separation. Newly developed molecular techniques provide additional information regarding their pathogenicity, patient survival and potential response to therapy. [16] Although numerous genetic alterations have been defined in human gliomas, unrevealing of loss of 1p/19q in oligodendroglial tumors and its association with prolonged survival and good chemotherapeutic response is nothing short of revolution. [3],[5],[6],[7],[17],[18],[19],[20],[21] In this regard, the current study was performed to analyze the frequency of 1p/19q deletion, p53 and EGFR proteins expression in various subtypes and grades of glial tumors, and to further understand the significance of these alterations in facilitating stratification of various subtypes. The combined 1p/19q loss is an important predictor of overall survival. [6] The good response of anaplastic OGs to chemotherapy is closely related to the presence of 1p and/or19q deletion. [5],[7],[22] The clinical implications of 1p and/or 19q loss in astrocytic tumors are however unclear. [6] MOAs have not been studied as extensively as regards their 1 p and 19 q deletion status. Previous studies show that OGs having astrocytic elements are less likely to harbor these favorable deletions. Moreover, even if they show the 'deletion' they are less likely to respond as favorably to chemotherapy. [23] Yet another study indicates that the mixed gliomas group can behave just as favorably as the OG group in the presence of 1p deletion. Maintz et al., suggested the existence of two genetic subsets of MOAs, one genetically related to ASs and the other genetically related to OGs. [19] They found MOAs with TP53 mutations to be more often AS-predominant, while those with chromosome 19 q loss were more often OG-predominant. Further studies are therefore warranted to explore the pathogenetic links between the MOAs and the pure OGs. [24] Distinction of the different types of gliomas on histopathological criteria alone can lead to interobserver diagnostic variability in individual cases. Frequency of combined 1p/19q loss varies from 44 to 67.9% in OGs, 26 to 31% in MOAs and is comparatively lower (8 to 25%) in ASs. Isolated 1 p and 19 q deletions have also been detected in all these three group of tumors. [5],[6],[10],[18],[25],[26],[27],[28] Reddy et al., studied 77 paraffin-embedded tissues using FISH for detecting 1p/19q loss. [28] Combined 1p/19q deletion was found in 65% OGs, 60% MOAs and only 25% of ASs. In the current study, majority (65%) of the OGs showed isolated/combined 1p/19q loss. Amongst the MOAs, 66.6% showed this alteration. However, none of the 14 cases of ASs showed deletion of either 1p or 19 q. Oligodendroglial phenotype was highly associated with isolated or combined 1p/19q loss ( P < 0.05). GFAP immunopositivity was noted in OGs and in the oligodendroglial component of MOAs, in the cytoplasm of the minigemistocytes and gliofibrillary oligodendrocytes in the form of perinuclear homogenous blobs. These cells may represent transitional forms between astrocytes and oligodendrocytes, or they may have a phenotype characteristic of a transient stage during oligodendroglial development. [29],[30],[31],[32],[33] The ASs showed a fibrillary staining pattern with GFAP. This pattern was also noted in the astrocytic component of the MOAs. Oligodendrogliomas are rare in children. Their molecular characteristics have not been well documented. There are only a few isolated studies, which suggest that pediatric OGs arise by molecular alterations distinct from adult OGs and so, therapy used in adults cannot be translated in pediatric cases. [14],[34] Raghavan et al., analyzed the 1p/19q status in 26 cases of pediatric OGs. [14] None of the 15 tumors that affected children below 9 years of age had 1p or 19q deletion. In tumors from children above 9 years, 1p loss was identified in 45% and 19q in 27% cases. They concluded that alterations on 1p or 19q are infrequent in pediatric compared to adult OGs and are virtually absent in OGs presenting in the first decade of life. Kreiger et al., used FISH assay to determine 1p/19q status in 10 cases of pediatric OGs and 3 pediatric MOAs. [34] Only one of their cases of OG harbored 1p loss, thus suggesting that pediatric OGs arise by molecular alterations distinct from adult OGs. In the present study, out of 29 cases with oligodendroglial differentiation, there were two pediatric cases-one pure OG and a MOA, both grade II. None of these harbored 1p/19q loss. However, both were p53 immunopositive. This, however, is too small a number for proper evaluation of pediatric cases, and more number of cases over the pediatric age range need to be evaluated. TP53 gene mutation as well as p53 protein expression is more common in astrocytic tumors as compared to the oligodendroglial tumors. von Deimling et al., found p53 gene mutation in 30-40% of ASs and anaplastic AS. [35] Hagel et al., found p53 mutation in 13.6%, 21.09% and 26.66% of grade II OGs, grade III OGs and in glioblastomas, respectively. [9] Nayak et al., documented p53 protein expression in more than 50% of astrocytic tumors. [36] Only 28% of their oligodendroglial tumors were p53 immunopositive. Though they did not find any correlation with the grade of astrocytic tumors, there was a trend of positive correlation with the grade in case of OGs. In contrast to TP53 mutation, p53 protein expression is more common and has been reported to range from 30 to 75% in OGs with conflicting results on its prognostic significance. [9],[37],[38],[39] It has been hypothesized that more frequent detection of p53 protein expression compared to TP53 mutation can be due to accumulation of aberrant p53 protein as a result of other mechanisms. Additionally, p53 expression has been found to be associated with a poor overall survival in patients with OGs and to increase with the grade of the tumor. Jeon et al., found 44.8% of anaplastic oligodendrogliomas (AOG) to be immunopositive for p53 as compared to 14.8% of low-grade oligodendrogliomas (LOG). [10] In the current study also, p53 immunopositivity was very rare in OGs, only 10% being p53 immunopositive, including 1 case each of grade II and grade III OG (2/20). In MOAs, p53 was immunopositive in 33% cases (3/9). Additionally, all the p53-positive OGs and MOAs showed only a weak (grade 1) staining intensity. In contrast, majority (57.1%) of ASs showed aberrant p53 protein expression (8/14), with the staining intensity being good-to-intense (grade 2-4) in most of the p53-positive cases (70%). Additionally, frequency of p53-protein expression was seen to increase with the grade of the tumor in all the three subtypes of glial neoplasms included in our study. Therefore, the current study confirms the earlier finding that OGs are less likely to show p53 protein overexpression as compared to ASs ( P = 0.018). Various studies have shown an inverse correlation between 1p/19q deletion and TP53 gene mutation. [7],[10],[19],[26],[40],[41],[42] In the present study, majority of the cases, which harbored either combined or isolated 1p/19q deletion, were p53 negative. Majority of the ASs were p53 immunopositive and none showed either combined or isolated loss of 1p/19q. Thus p53 protein overexpression and 1p and/or 19q loss appear to be mutually exclusive events. Amplification of EGFR gene appears mainly in adult primary glioblastomas. [43] Interestingly, in a study by Reifenberger et al., nearly 50% of both WHO grade II and grade III OGs showed strong EGFR mRNA and protein expression in the absence of EGFR gene amplification. [11] Reis-Filho et al., found EGFR immunoexpression in 100% of their OG cases. [44] In the present study, most of the OGs (85%) and MOAs (77.7%) showed a diffuse lace-like immunopositivity for EGFR, which was helpful in highlighting even small foci of oligodendroglial differentiation in difficult cases of MOA. None of the astrocytic tumors (Grades II and III) and astrocytic areas in MOA was immunopositive. The results were statistically significant ( P< 0.05). To summarize, majority of the oligodendrogliomas and oligoastrocytomas that showed combined or isolated loss of 1p/19q were p53 negative and showed diffuse lace-like immunopositivity for EGFR protein. None of the astrocytic tumors (Grades II and III) showed 1p/19q alteration or EGFR expression, and majority showed good to intense p53 immunopositivity. There were two pediatric oligodendroglial tumors, both of which lacked 1 p/19 q alterations. Moreover, 1 p/19 q loss and p53 immunoexpression were mutually exclusive. It is essential to correctly diagnose OG as they are chemosensitive and have been associated with an overall better outcome. [5],[6],[7] However, no specific marker is available for OG and GFAP labels both ASs and OGs. Thus, although histopathology is the mainstay in the diagnosis and subtyping of glial tumors, the present study suggests that use of relevant molecular techniques and immunohistochemical markers should be integrated in the routine diagnostic setup as the judicious use of a panel of selected markers is unquestionably helpful in diagnostically ambiguous cases. This is significant in view of the better survival and response to chemotherapy associated with tumors exhibiting oligodendroglial differentiation. The present study has limitations especially lack of follow-up and hence, prognostic correlation. Also the number of pediatric cases is too small for any definitive conclusion, regarding their molecular markers. However, this is the first study from India on molecular phenotyping of gliomas, with special emphasis on oligodendroglial tumors and more such studies with larger number of cases are required. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09164f2.jpg] [ni09164t2.jpg] [ni09164t4.jpg] [ni09164t3.jpg] [ni09164t1.jpg] [ni09164f1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}