 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
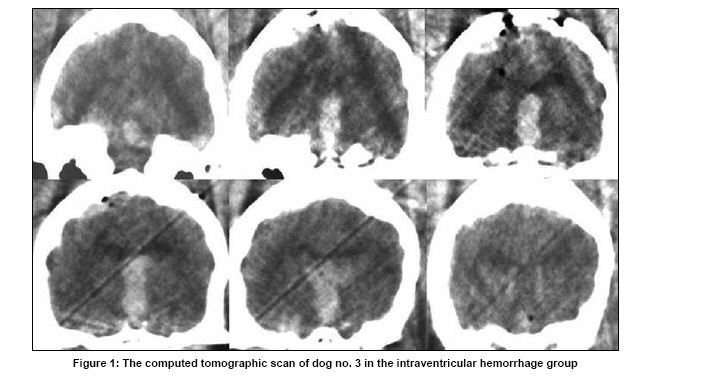
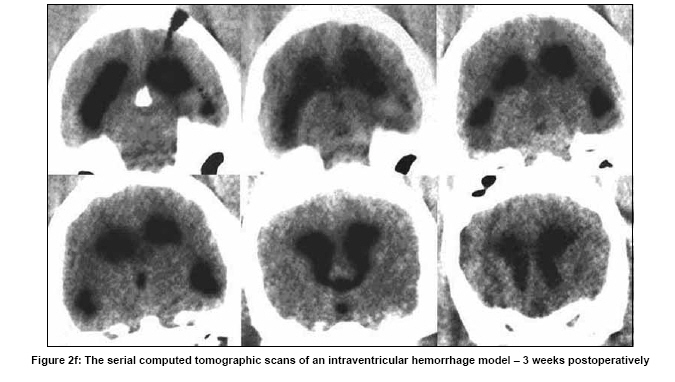
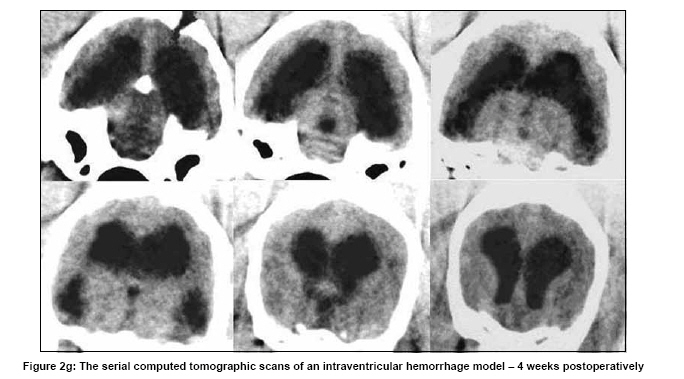
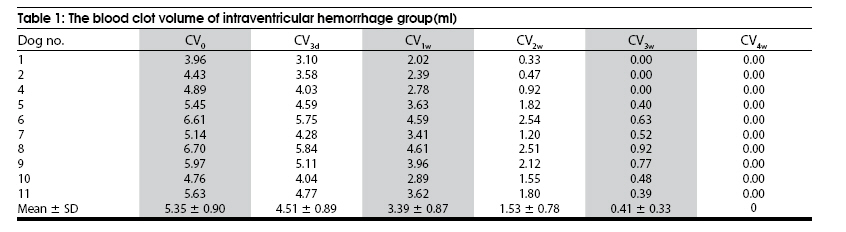
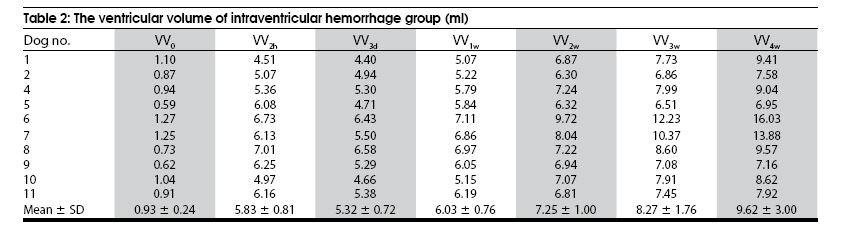
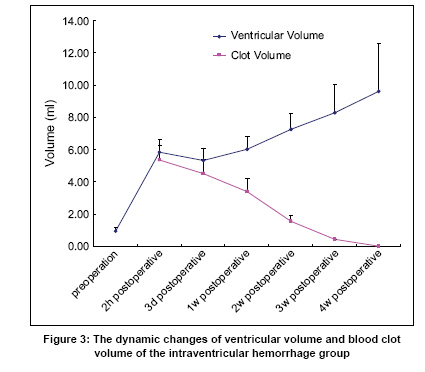
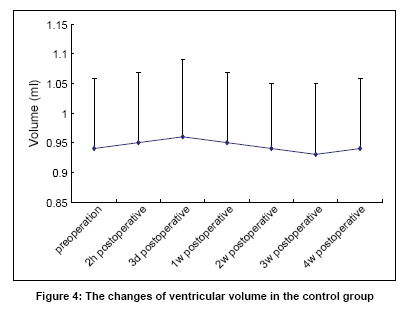
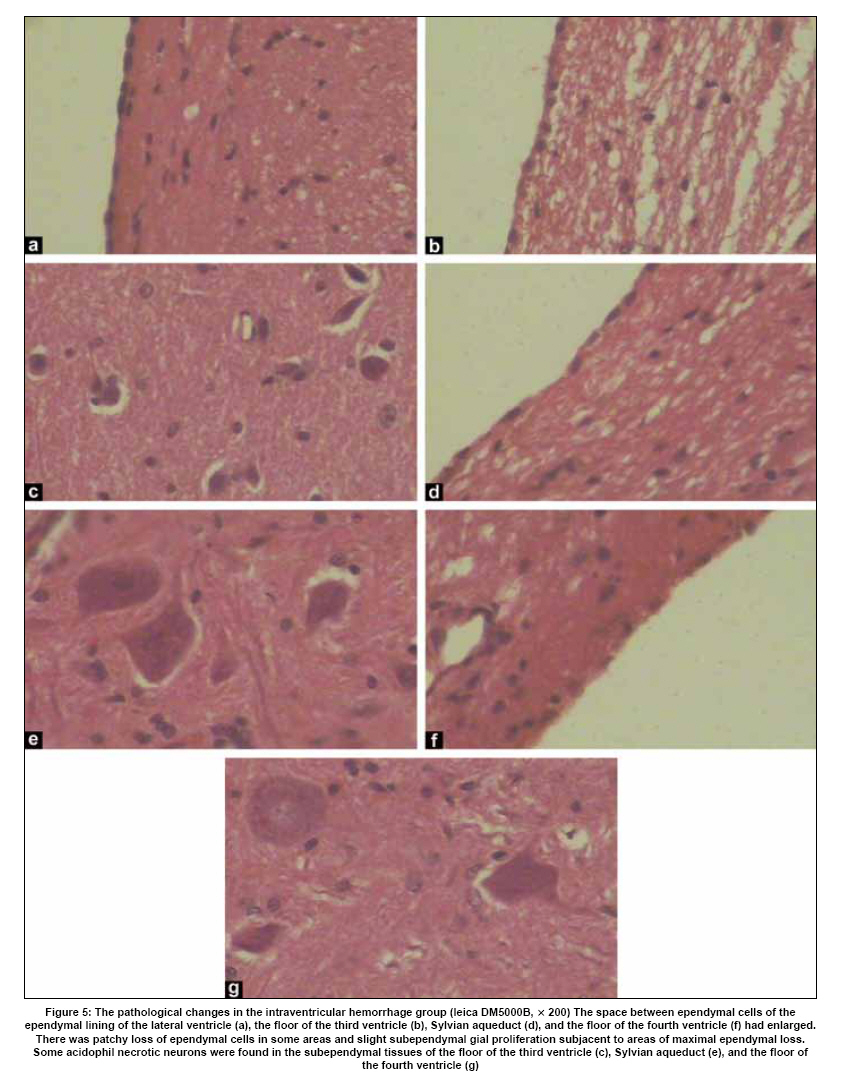
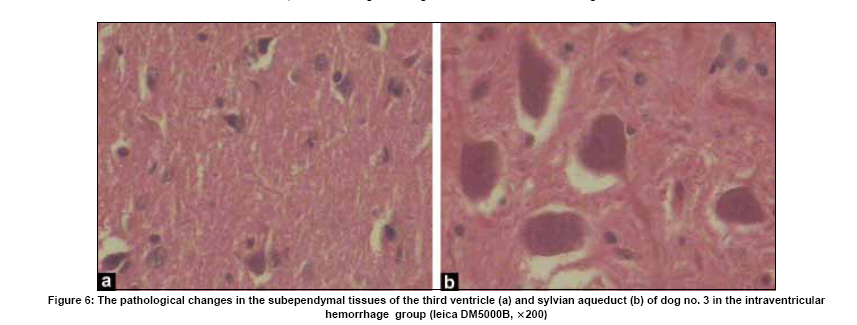
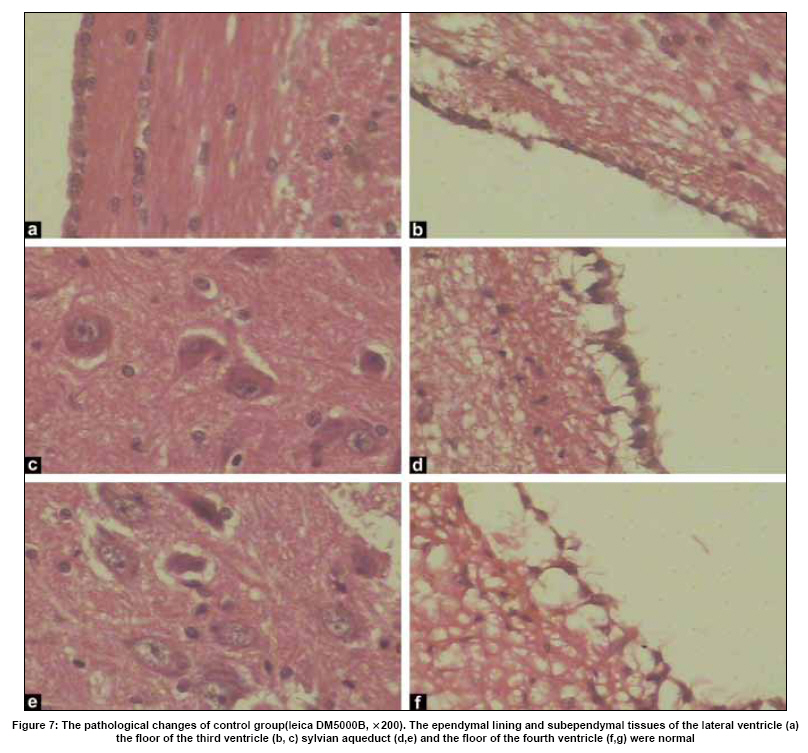
Neurology India, Vol. 57, No. 5, September-October, 2009, pp. 567-577 Original Article The mechanism of pathological changes of intraventricular hemorrhage in dogs Jiong Dai, Shanquan Li, Xiaoxiong Li, Wenhao Xiong, Yongming Qiu Department of Neurosurgery, Renji Hospital, Shanghai, China Date of Acceptance: 14-Feb-2009 Code Number: ni09165 PMID: 19934554 DOI: 10.4103/0028-3886.57798 Abstract Background : Intraventricular hemorrhage (IVH) is an independent risk factor for both morbidity and mortality in patients with intracerebral hemorrhage and subarchnoid hemorrhage. The pathophysiological mechanisms by which blood within the ventricles causes brain damage are still poorly understood.Settings and Design : We developed a canine (dog) model with long-term survival. Aims : To study the mechanisms of pathological changes associated with IVH. Materials and Methods : The neurological status, cranial computed tomographic findings, and the pathological changes were studied in the dogs with IVH and also in the control dogs, intraventiricular saline injection. Results : In all the dogs in the control group there were no abnormalities in all the three parameters studied. The dogs in the IVH group developed neurological deficits after the blood injection. There was linear relationship between the ventricular volume and blood clot volume in the first week. After the first week, there was progressive enlargement of the ventricular volume, while the clots continued to shrink. There was complete lysis of the clots within 4 weeks. Pathological studies showed distruction of the ependymal lining of the ventricular system, subependymal gliosis and ischemia of the neurons in the subependymal areas, prominently around the aqueduct. Conclusion : Ventricular dilation was the prominent feature following intraventricular injection of the blood. The other pathological features included disruption of ependymal lining, subependymal gliosis, and ischemic necrosis of neurons in the periventricular tissue of the third ventricle, aqueduct, and the fourth ventricle. These pathological may have some role in the ventricular dilatation following IVH. Keywords: Animal model, intraventricular hemorrhage, pathophysiological mechanism Introduction Spontaneous intracerebral hemorrhage (ICH) and aneurysmal subarachnoid hemorrhage (SAH) may be associated intraventricular hemorrhage (IVH) [1] and it is an independent risk factor for both morbidity and mortality. [2],[3],[4],[5],[6],[7],[8],[9],[10],[11] In patients with ICH and IVH, 20 ml of blood in the ventricles is a lethal volume. [8] However, the pathophysiological mechanisms by which blood within the ventricles causes brain damage are still poorly understood. Recent studies have demonstrated that accelerated clearance of IVH and rapid normalization of ventricular volume can be achieved by intraventricular administration of the thrombolytic agents, urokinase or recombinant tissue plasminogen activator (rtPA). [12],[13],[14],[15],[16],[17],[18] In this study, we developed a canine (dog) model of IVH with long-term survival and elucidated the possible mechanisms leading to brain damage in IVH. Materials and Methods The experimental protocols were in conformity with the national law for the protection of animals. Animals Sixteen adult mongrel dogs of either gender, each weighing 10 to 17 kg, were used for this study. They were randomly allocated to two groups: (1) IVH group-11 dogs and (2) control group-5 dogs. IVH group received intraventricular blood injection and control group received intraventricular saline injection. Operative procedure Preparation Animals were fasted for 12 hours pre-operatively. After general anesthesia, with intra-abdominal injection of 2.5% thiopental sodium in a dosage of 25 mg/kg and a subcutaneous injection of atropine in a dosage of 0.4 mg, the animals were intubated and ventilated with a 5:3 mixture of nitrous oxide and oxygen. Ventilation was adjusted to maintain arterial CO 2 pressure between 35~45 mmHg. A femoral arterial cannula was secured to be connected to the multichannel physiological monitor. Arterial blood pressure and blood gas were monitored. The animals were infused with 500 ml of saline, 20 mg of diazepam, and 16 x 10 4 U of gentamycin. The dosage of diazepam was no more than 2 mg/min. Nine milliliters of blood was withdrawn from the femoral arterial catheter and the syringe containing the blood was placed in a metal basin containing warm sterile saline. Surgical technique The head of the dog was fixed on a stereotactic frame with bilateral external auditory metal bars at the zero point. The body of the lateral ventricle was identified by the stereotactic coordinates: Transverse = 8 mm, vertical = 25 mm, and rostral = 20 mm. The puncture depth was regulated to 20 mm from the outer table of the cranial skull. A ventricular catheter was placed in the right lateral ventricle with the catheter tip lying within the body of the ventricle. Dogs in the IVH group were injected 9 ml of prepared autologous arterial blood into the right lateral ventricle via the ventricular catheter over a period of 30 minutes. Dogs in the control group received the same volume of sterile saline. Precaution was taken during the procedure not to inject air. The vital signs, eyelash reaction, and pupil reaction were monitored for any herniation signs in all the dogs. Following the procedure, the dogs were awaken from anesthesia. Postoperative evaluation Neurological status The neurological status of all the 16 dogs was evaluated both pre-operatively and daily, post-operatively. We used a four scale system: Grade I = normal; Grade II = drowsy, difficult standing, and reduction in muscle force; Grade III = stupor, slight movement in the limbs, swallowing for liquid; Grade IV = comatose, paralysis, no swallowing movement. Cranial computed tomographic scans Cranial computed tomography (CT) scan was done in all the dogs pre- operatively and at 2 hours, 3 days, 1 week, 2 weeks, 3 weeks, and 4 weeks post-operatively. The dogs were sedated with intra-abdominal injections of 2.5% thiopental sodium in a dosage of 20 mg/kg and scanned by Picker scanner (Model 2000, Picker Inc. U.S.A.). Non overlapping contiguous coronal cuts with a constant collimation width of 3 mm were made to include the entire ventricular system. The image data was fed into a computer with a digital camera (Olympus 2020) and analyzed with SigmaScan Pro Image Analysis Program (Version 5.0.0, SPSS Inc., Chicago, IL) to calculate the ventricular volume and blood clot volume. Because of the artifacts of posterior cranial fossa, the fourth ventricular volume and fourth ventricular blood clot volume could not be measured ideally and were excluded from further analysis. Pathological studies At the end of 4 weeks, all the animals were intubated and anesthetized deeply with intra-abdominal injections of 2.5% thiopental sodium after confirmation of normal arterial blood gas values. The animals were then sacrificed with intravenous potassium chloride. The brain was fixed by perfusioning 4% paraformaldehyde through the common carotid arteries. After fixation for a period of 2 hours, the brain was removed intact from the cranium and fixed in 4% paraformaldehyde solution for 2 weeks. The ependymal and subependymal tissues from the lateral ventricle, the floor of the third ventricle, aqueduct, and the floor of the fourth ventricle were taken for histological examination. Statistical analysis The data were presented as mean±SD and one- way ANOVA and linear regression analysis were done. A value of P < 0.05 was considered statistically significant. All data were analyzed with SPSS, version 13 for windows (SPSS Inc., Chicago, IL). Results Neurological status All the 16 dogs were neurologically normal (Grade I) preoperatively. Intraventricular hemorrhage group During blood injection, there was a transient and slight increase in blood pressure, but was still within normal range. Eyelash and pupil reaction were present throughout the procedure. In the dog no. 3 the CT scan done at 2 hours post-operatively showed blood filling the entire third ventricle and the third ventricle was dilated [Figure - 1]. The neurologic status in this dog after blood injection was Grade IV for 36 hours and then improvement to Grade III. On the third post-operative day, the dog lapsed into coma and died. The data of this dog was excluded from the statistical analysis. However, the brain was fixed and removed for pathological study. The neurologic status of dogs no. 6, 8, and 11 remained in Grade IV for 24 hours post-operatively. The other 7 dogs were well oriented 12 hours after blood injection. All 10 dogs recovered to Grade I within±days post-operatively and remained neurologically stable during the 4-week follow-up period. The only neurologic deficit was gait unsteadiness. Control group Six hours after sterile saline injection, all the 5 control dogs recovered from anesthesia to Grade I and were neurologically normal during the 4-week follow-up period. Cranial computed tomographic scans The CT scans done pre-operatively in all the 16 dogs showed the normal slit-like ventricle. The ventricular volume and blood clot volume were measured preoperatively and at 2 hours, 3 days, 1 week, 2 weeks, 3 weeks, and 4 weeks postoperatively and designated as VV 0 , VV 2h , VV 3d , VV 1w , VV 2w , VV 3w , VV 4w , CV 0 , CV 3d , CV 1w , CV 2w , CV 3w , and CV 4w . Intraventricular hemorrhage group Preoperative ventricular volume (VV 0 ) was 0.93±0.24 ml [Figure - 2]a. After blood injection, the initial ventricular blood clot volume (CV 0 ) varied from 3.96 to 6.70 ml with a mean of 5.35±0.90 ml and VV 2h was 5.83±0.81 ml. VV 3d was 5.32±0.72 ml, CV 3d was 4.51±0.89 ml, VV 1w was 6.03±0.76 ml, and CV 1w was 3.39±0.87 ml [Figure - 2]b. The linear regression value was significant: VV 2h against CV 0 (b 5 0.87, P 5 0.00001), VV 3d against CV 3d (b 5 0.69, P 5 0.002) and VV 1w against CV 1w (b 5 0.75, P 5 0.001). The ventricular volume contracted as the blood clot volume dissolved in the first week post-operatively [Figure - 2]c and d. But after the first week, the ventricular volume progressively increased while the blood clot volume decreased. The blood clots dissolved completely within 4 weeks post-operatively [Figure - 2]e, f, g. [Table - 1] and [Table - 2] show the details of blood clot volume and ventricular volume in the IVH group [Figure - 3]. Based on the early neurologic status at 24 hours the dogs with IV blood injection were grouped into two groups: Group 1 (dog nos. 6, 8, and 11) and Group 2: (all other 7 dogs). The CV 0 for Group 1 and Group 2 were 6.31±0.59 ml and 4.94±0.66 ml, respectively and the corresponding VV 2h were 6.63±0.43 ml and 5.48±0.68 ml, respectively. Comparisons of CV 0 and VV 2h between the two groups showed statistically significant differences (P CV0 = 0.015 and P VV2h = 0.028), implying that the initial blood clot volume in the ventricles was one of the main factors impacting the early neurological status. VV 4w /VV 0 , which represented the degree of ventricular dilatation, was 10.40±1.83. The linear regression of VV 4w /VV 0 against CV 0 was significant (b 5 1.71, P 5 0.002). Control group The ventricular volume of all 5 dogs in the control group remained normal after sterile saline injection for the 4-week follow-up period. [Table - 3] shows the details of the ventricular volume in the control group [Figure - 4]. Pathological studies Intraventricular hemorrhage group No blood clot was found in the ventricles of all 10 dogs' brains in the IVH group. The space between the ependymal cells of the ependymal lining of the lateral ventricle, the floor of the third ventricle, the aqueduct, and the floor of the fourth ventricle was enlarged. There was a patchy loss of ependymal cells in some areas and slight subependymal gial proliferation in areas of maximal ependymal loss. There were ischemic neurons in the subependymal tissues of the floor of the third ventricle, aqueduct, and the floor of the fourth ventricle. These cells were triangular in shape. Their cytoplasma was easonophilic, and their nuclei disappeared. These pathological changes were most prominent in the tissues surrounding the aqueduct [Figure - 5]. Ischemic neurons were more in the subependymal tissues of the third ventricle and aqueduct in the Dog no. 3, whose CT scan done 2 hours post-operatively showed casting of the third ventricle with blood clots [Figure - 6]. Control group In the control group, the ependymal lining and subependymal tissue of the lateral ventricle, the floor of the third ventricle, aqueduct, and the floor of the fourth ventricle were normal [Figure - 7]. Discussion Ventricular dilation following IVH is a common complication and is associated with poor outcomes. [19],[20] The outcomes are much worse when the third and/or fourth ventricle are dilated and casted with blood. [13],[20] Clinical and experimental studies suggest that the ventricular dilatation following IVH may be due to 1) the impaired CSF circulation and absorption and 2) the mass effect of blood clot on the ventricular wall. [11],[19],[20],[21] An effective IVH animal model would be extremely useful to study the pathophysiology of IVH and also for testing new treatment strategies. Only a very few experimental models of IVH have been developed. Pang, et al., [22] developed an IVH model in dogs by intraventricular injection of 9 ml of solid autologous blood and in this model it took 38 to 65 days for complete lysis of blood in the ventricles. An IVH model in pigs was developed by intraventricular injection of 10 ml of blood mixed with thrombin. In this model the ventricular volume returned to normal values within±weeks by complete clot resolution. [11] Lodhia, et al., [23] developed an adult rat model of IVH by injecting 0.2 ml of arterial blood into the lateral ventricle. There was almost complete clot resolution within one week. In humans follow-up CT studies have shown that it takes three weeks for the resolution of intraventricular hemorrhage to disappear. [24] In our model intraventricular blood injection was associated with ventricular dilatation and it took four weeks for the blood clot in the ventricles to dissolve completely. Our model closely simulates the situation in human IVH. In our model the initial intraventricular blood clot volume (CV 0 ) was 5.35±0.90 ml, much less than the injected 9 ml of blood. The following factors might explain this discrepancy: 1) The volume of blood clot created from 9 ml of whole blood was probably less than 9 ml, 2) the blood clot in the fourth ventricle was excluded from the measurement of clot volume, and 3) some of the blood clot might have gone into the basal cistern. In the earlier experimental models such phenomenon has been observed. [11],[22] Within the first week after blood clot injection, there was linear relationship between the ventricular volume and the blood clot volume. These observations suggest that in the early stages of IVH the ventricular dilatation may be related to the mass effect of blood clot on the ventricular wall. After one week there was progressive increase in the ventricular volume while there was decrease in the volume of the blood clot. Probably the ventricular dilatation at this stage may be due to impaired cerebrospinal fluid circulation and absorption. In the dogs in the IVH group there was destruction of the ependymal lining of the ventricular system and subependymal glial proliferation.These changes might be the result of the mechanical effect of blood clot distending the ventricular walls and the toxic effect of thrombin to the ependymal cells. [25] These pathological changes may cause reduced compliance of the periventricular tissue and would prevent the periventricular tissues from recoiling, leading to ventricular dilatation. This may be the other mechanism for the progressive ventricular dilatation seen in the the IVH dogs after the first week. In the dogs in the IVH group there were ischemic changes in the neurons in the periventricular tissues of the third ventricle, aqueduct, and the fourth ventricle. These changes were more pronounced in the periaqueductal tissue. In the Dog no. 3, in whom third ventricle was casted with blood clot and dilated, there were more ischemic neurons in the subependymal tissue of the third ventricle and aqueduct. This dog died early in the course of the experiment. The pathogenesis of ischemic changes in the neurons may be due to: 1) A decrease in cerebral blood flow in the periventricular tissue because of mechanical compression by the ventricular volume on the periventricular perforating vessels, 2) possible reduction in the number of capillaries in the periventricular tissue as a result of ventricular dilatation, [ 26] 3) reduced cerebral perfusion pressure due to increased intracranial pressure after IVH and 4) vasospasm rarely associated with IVH. [27],[28],[29],[30] References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09165f2g.jpg] [ni09165f2f.jpg] [ni09165f2e.jpg] [ni09165f4.jpg] [ni09165f6.jpg] [ni09165f5.jpg] [ni09165t1.jpg] [ni09165f3.jpg] [ni09165t2.jpg] [ni09165f2b.jpg] [ni09165f2a.jpg] [ni09165f2c.jpg] [ni09165f2d.jpg] [ni09165t3.jpg] [ni09165f7g.jpg] [ni09165f7.jpg] [ni09165f1.jpg] |
| |||||||||

{kind=link}
![Figure - 2]a](/showimage?ni/photo/ni09165f2a.jpg){kind=link}
![Figure - 2]b](/showimage?ni/photo/ni09165f2b.jpg){kind=link}
![Figure - 2]c](/showimage?ni/photo/ni09165f2c.jpg){kind=link}
![Figure - 2]e](/showimage?ni/photo/ni09165f2e.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}