 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
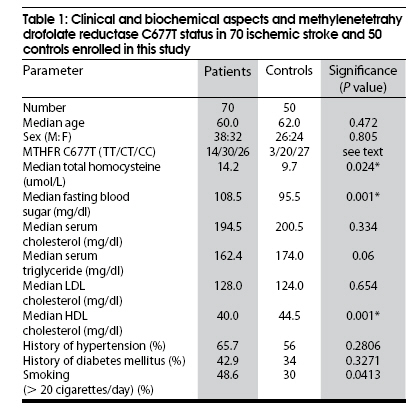
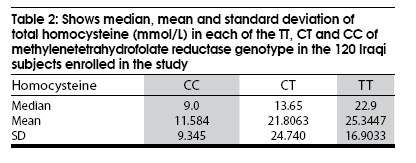
Neurology India, Vol. 57, No. 5, September-October, 2009, pp. 631-635 Brief Report Methylenetetrahydrofolate reductase C677T polymorphism in Iraqi patients with ischemic stroke Nasir A. S. Al-Allawi, Arteen S. Avo1 , Jaladet M. S. Jubrael 2 Department of Pathology, College of Medicine, 1 Azadi Teaching Hospital, 2 Scientific Research Center, University of Dohuk, Iraq Date of Acceptance: 02-Jul-2009 Code Number: ni09176 PMID: 19934565 DOI: 10.4103/0028-3886.57821 Abstract Background: Data are conflicting concerning the association between ischemic stroke and methylenetetrahydrofolate reductase (MTHFR) C677T mutation. Studies addressing this matter in developing countries are limited.Aim: This study was undertaken to evaluate MTHFR C677T gene polymorphism as a possible risk factor in patients with ischemic stroke in Iraq. Settings and Design: A case-control study in a major teaching hospital in Northern Iraq. Materials and Methods: Study population included 70 patients with ischemic stroke diagnosed by computed tomography (CT) or magnetic resonance imaging (MRI) and 50 controls matched by age and sex. All the patients and controls had detailed neurologic examination and blood sugar, lipid profile, total homocysteine, as well as, MTHFR gene analysis. The MTHFR C677T mutation status was detected in the amplified products using reverse hybridization to specific mutant and wild oligonucleotide probes by a colorimetric microwell plate method. Statistical Analysis: Mann-Whitney U test and Chi-square tests were used to find the significance. Results: The median age of the patients was 60 years and 54% were males. The MTHFR C677T gene analysis detected TT genotype in 20% of patients and in 6% of controls and CC genotype in 37% of the patients and in 54% of the controls. The calculated risk of ischemic stroke in the subjects with TT genotype was 4.85 times more than the subjects with CC genotype (P=0.03). Serum homocysteine level was significantly higher in the patients than the controls (P=0.02). The serum homocysteine levels were significantly higher in those with TT and CT genotypes when compared to those with CC genotype (P < 0.001 and P=0.04, respectively). Conclusion: In the Iraq population studied MTHFR C677T TT genotype was a significant risk factor for ischemic stroke and it was related to the increased total homocysteine levels and the risk for ischemic stroke was graded with increasing MTHFR 677T allele dose. Keywords: Homocysteine, ischemic stroke, methylenetetrahydrofolate reductase C677 T Introduction Ischemic stroke is a major cause of morbidity and mortality in developed countries, and World Health Organization (WHO) anticipates similar trends in developing countries within the next decade. [1] Stroke prevention should be one of the immediate priorities of health authorities in developing countries. Several modifiable risk factors have been identified and would be suitable targets for intervention; one of them is total homocyteine concentration, though the data is controversial. [2] Hyperhomocyteinemia may be acquired or inherited and the frequent inherited cause is the methylenetetrahydrofolate reducatase (MTHFR) C677T mutation. This mutation is responsible for Ala223Val substitution in a highly conserved residue of the molecule, rendering the enzyme thermolabile and leading to hyperhomocysteinemia, particularly in homozygous individuals. [3] The worldwide prevalence of MTHFR C677T mutation in its homozygous state is variable and ranges between 8% and 18% in Europe and Northern America. The mutation is uncommon in Africans and people of African origin. [4] Studies from Asian countries reported variable frequencies: 11% in Japanese and Chinese and 0-1.2% in Indians. [4],[5],[6],[7] The reported frequency in the studies from Eastern Mediterranean region range between 5.1% and 18%. [8],[9],[10] A recent study from Iraq revealed a frequency of 8% among healthy blood donors. [11] There are no studies addressing the relation between MTHFR C677T mutation and ischemic stroke from Iraq. Materials and Methods Of the 83 consecutive patients with ischemic stroke attending Azadi Teaching Hospital, Dohuk, Iraq, between December 2005 and April 2007, 70 patients were recruited for this study. The inclusion criteria was ischemic stroke confirmed by magnetic resonance imaging (MRI) and/or computer tomography (CT). Patients with renal disease, cardioembolic stroke, malignancy, and pregnant women were excluded. During the same period, 50 age and sex matched healthy subjects attending the outpatient laboratory of the hospital for routine general checkup with no history of venous or arterial thrombosis were recruited as controls. The study was approved by the ethical committee at the College of Medicine, and informed consent was obtained from all enrollees. All the patients had a detailed history and neurologic examination, Based on neuroimaging findings, patients were categorized into lacunar or nonlacunar stroke according to criteria by Ohira et al. [12] All patients and controls had fasting blood sugar and lipid profile (Biomereaux, France). Serum total homocystiene was Estimated using enzymatic assay (Diazyme laboratories, Germany), [13] with an automatic analyzer (TARGA 3000, Biotanica instruments, Italy). Blood collected in the EDTA vial was frozen within one to two hours at -208, and kept for DNA extraction, DNA was extracted within three months of sample collection using a phenolchloroform method and was amplified using a Primus 25 thermocycler (MWG-Germany) with specific primers (ViennaLab, Austria) and a cycling program consisting of pre-polymerase chain reaction (PCR) at 94°C for 2 minutes, followed by 30 cycles at 94°C for 15 sec; 58°C for 30 sec; 72°C for 30 sec, and a final extension of 3 minutes at 72°C. The MTHFR C677T mutation status was detected in the amplified products using reverse hybridization to specific mutant and wild oligonucleotide probes by a colorimetric microwell plate method, [14] according to the manufacturer's instructions (ViennaLab, Austria). Statistical analysis was done using SPSS software package. Mann-Whitney U tests and Chi square tests were used whenever appropriate and a P < 0.05 was considered significant. Results The median age of the patients with ischemic stroke was 60 years (male : female: 1.19:1) and for the controls 62 years (male : female: 1.08:1). Of the 70 patients with ischemic stroke, 12 patients had lacunar infarct and the remaining 58 had nonlacunar infarct. [Table - 1] shows the distribution of MTHFR C677T genotypes [TT Homozygous; CT Heterozygous; and CC wild type] in patients and controls with relevant clinical and biochemical data. TT genotype was detected in 20% of patients and 6% of controls, while CC genotype was detected in 37% of patients and 54% of controls. The calculated risk of ischemic stroke in the subjects with TT genotype was 4.85 fold (95% CI: 1.14-28.73) higher than the subjects with CC genotype, ( P = 0.03). The median serum homocysteine levels in patients with ischemic stroke was 14.2 μmol/L (mean, 20.9 + 22.2) where as the median levels in controls was 9.7 μmol/L (mean 12.3 + 10.2) (P = 0.02). Highest homocysteine levels were found in those with TT genotype and the homocysteine levels were significantly higher than in those with the CC genotype, but not in those with the CT genotype ( P < 0.001 and 0.06, respectively). Furthermore, homocysteine levels were also significantly higher in CT compared to CC genotype ( P = 0.04) [Table - 2]. No significant differences were found in age, sex, MTHFR C677T mutation status, total homocysteine levels or other biochemical studies between patients with lacunar stroke and nonlacunar stroke. However, history of hypertension and smoking were significantly higher among patients with lacunar infarct ( P = 0.001 and 0.02, respectively). Discussion The study suggests that in Iraq population the risk of ischemic stroke Is about five fold higher in subjects homozygous for MTHFR C677T (TT genotype) gene mutation when compared to those homozygous for the wild gene (CC genotype). Recent meta-analysis including 13,928 subjects, showed similar high significant overall pooled odds ratio for stroke in subjects with the TT genotyped when compared to the CC genotype, 1.26 (95% confident intervals (CI), 0.56 to 17.92). [15] Another meta-analysis, including 14,870 subjects showed a graded increase in ischemic stroke risk with increasing MTHFR 677T allele dose. [16] Some of the case-control studies from China and Japan showed similar significant increased risk of ischemic stroke in TT genotype. [17],[18] While studies from India did not find such significant association though TT genotype was more frequent in the patients with ischemic stroke. This is probably related to the low prevalence of TT genotype in the general population. [6],[7],[19],[20],[21] One hospital based study from India reported the probability of carrying the mutant allele (TT or CT genotypes) at 22.29 fold higher in patients than controls. [22] In our study total serum homocysteine was significantly higher in subjects with TT and CT genotypes. Similar were the findings in the meta-analysis including 16849 subjects. [23] Case control studies from Asia, also confirm our observations. [6],[17],[18] Casas and Coworkers [15] demonstrated that the actual increase in the risk of stroke in homozygous (TT) individuals was close to that predicted from the difference in homocysteine level conferred by this variant. This concordance is consistent with a casual relation between homocysteine and ischemic stroke. [15] Such a correlation between serum total homocysteine levels and C677T MTHFR mutation is quite expected, since MTHFR catalyzes the reduction of 5,10 MTHF to 5 MTHF, the predominant circulatory form of folate and carbon donor for the remethylation of homocysteine to methionine and MTHFR C677T leads to a reduced MTHFR activity and thus elevated homocysteine. [24] In this case-control study significantly higher serum total homocysteine levels were observed in patients with ischemic stroke. Similar were the observations in other case control studies and also in some of the prospective studies. [17],[20],[25],[26],[27],[28],[29] This association with elevated homocysteine levels was stronger in case control studies than the association observed in the prospective studies, This discrepancy may partly be explained as elevated homocysteine levels may be a reflection of an acute phase reaction. [30] In the present study homozygous MTHFR mutation (TT) was associated with higher serum total homocysteine levels and also with the high risk for ischemic stroke. This would probably indicates that high levels of serum total homocysteine is a risk factor for ischemic stroke. These observations are supported by the meta-analyses using mendelian randomization, to assess the consistency between risk estimates obtained from genotype-disease studies and phenotype-disease studies, relating to the MTHFR mutation, homocysteine and the risk of ischemic stroke, which showed a causal relationship between homocysteine and ischemic stroke. [15] The precise mechanisms underlying the apparent adverse effect of hyperhomocysteinemia on the risk of the ischemic stroke are not clear, although several mechanisms have been proposed. Hyperhomocysteinemia may cause a rise in arterial blood pressure and thus increase the risk of ischemic stroke. [28] Another possible mechanism is that elevated total serum homocysteine induces oxidative injury to vascular endothelial cells and impairs the production of nitric oxide, a strong vasodilator, from the endothelium. [31] Hyperhomocyteinemia has been shown to enhance platelet adhesion to endothelial cells [32] and also to promote growth of vascular smooth muscle cells. [33] Hyperhomocysteinemia is associated with higher levels of prothrombotic factors such as b- thromboglobulin, tissue plasminogen activator, and factor VIII: C. [34] Confirming a causal relationship between elevated homocysteine and stroke is of clinical importance as serum homocysteine could be lowered by the B vitamin supplementation (folic acid, B12 and B6). [35] But the real challenge is to show that lowering homocysteine lowers the risk of stroke or death. Several trials have been done to address this issue. [36],[37],[38],[39] and some more studies are under way the results of which are awaited. [40],[41] One of the major limitations of our study was that we had not done a detailed nutritional status evaluation of both the patients and controls. We had also not done the folate, B12 and B6 status. These limitation emphasize the need for future studies to determine the folate, B12 and B6 status, in conjunction with serum total homocyteine and MTHFR C677T genotypes, in healthy subjects and patients with ischemic stroke in Iraq. Such data is important to plan national programs for possible preventive intervention. Acknowledgment Authors acknowledge with gratitude the critical review of the manuscript by Professor Michael Hughson (Emeritus Professor of Pathology, University of Mississippi Medical Center, US). References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09176t1.jpg] [ni09176t2.jpg] |
| |||||||||


{kind=link}
{kind=link}