 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
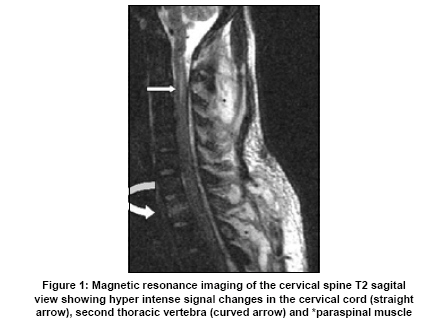
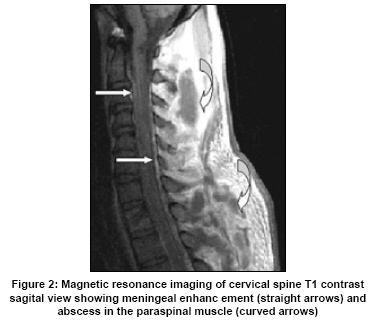
Neurology India, Vol. 57, No. 5, September-October, 2009, pp. 653-656 Case Report Community-acquired methicillin-resistant Staphylococcus aureus pyomyositis with myelitis: A rare occurrence with diverse presentation Girish Baburao Kulkarni, P. K. Pal, H. B. Veena Kumari 1 , M. Goyal, J. M. E. Kovoor 2 , Savitha Nadig3 , Gayathri Arakere3 Departments of Neurology, 1 Neuromicrobiology and 2 Neuroradiology, National Institute of Mental Health and Neurosciences (NIMHANS), Hosur Road, Bengaluru, Karnataka - 560 029, and Date of Acceptance: 02-Jul-2009 Code Number: ni09182 PMID: 19934571 DOI: 10.4103/0028-3886.57809 Abstract Staphylococcus aureus is the most common bacterial pathogen implicated in pyomyositis. There are increasing reports of community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) infections. The present case report brings out the diverse clinical manifestations of MRSA infection in the form of paraspinal pyomyositis, myelitis, spinal osteomyelitis, and pneumonia. Molecular typing of the organism confirmed the diagnosis. Patient was successfully treated with vancomycin and surgical drainage. Consideration of the possibility of methicillin-resistance and appropriate antibiotic selection is vital in the treatment of serious community-acquired staphylococcal infections.Keywords: Community-acquired methicillin-resistant Staphylococcus aureus, MRSA septicemia, myelitis, osteomyelitis, pyomyositis, vancomycin Introduction Pyomyositis is a rare primary muscle infection that is due to transient bacteremia, and Staphylococcus aureus is the most common organism isolated. [1] Community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) pyomyositis is being increasingly reported in the literature. In this case report we describe an interesting patient of CA-MRSA presenting with pyomyositis, and other sites of involvement who made a complete recovery with vancomycin and surgical drainage. Case Report A 19-year-old plumber was brought to our hospital with one-week history of intermittent fever, pain in the nape of the neck and back. Five days prior to the presentation he had worked for about 12 hours in cleaning an underground water tank. No past history of diabetes, alcoholism, malignancy, intravenous drug use, and human immunodefiency virus (HIV) infection was noted. On examination, he was febrile with temperature of 398C, there was redness and tenderness over the skin covering the cervical and thoracic spines. Liver was palpable four centimeters below the right costal margin and chest auscultation revealed crepitations over both lungs. Neurologically he was conscious and had no deficits. Investigations showed: Erythrocyte sedimentation rate of 85mm first hour (normal < 20 mm/hr); white blood cell (WBC) count of 14,200/cmm (normal < 12,000/cmm); creatinine kinase of 1,640 U/L (normal 15-160U/L); and serum for HIV 1 and 2 antibodies were negative. X-ray chest showed picture of bilateral bronchopneumonia. A provisional diagnosis of pyomyositis involving the paraspinal muscles and septicemia was considered and blood was sent for cultures. He was empirically started on parenteral ampicillin, amickacin, ceftriaxone, and metronidazole in the dosages recommended for the septicemia. Surgical drainage was not considered because there was no softening or pus pointing over the paraspinal area. Over the next three days he developed weakness in all the four limbs (2/5 proximally, 4/5 distally in upper limbs, and 2/5 distally in the lower limbs), with urinary retention. The deep tendon reflexes were absent in the upper limbs and exaggerated in the lower limbs, with extensor plantars bilaterally. Magnetic resonance imaging (MRI) of whole spine [Figure - 1] and [Figure - 2] was done, which showed extensive necrosis of the cervical, thoracic paraspinal group of muscles, with abscess formation. There was diffuse enhancement of the meninges in the cervical area with and T2 hyperintensities in the cervical spinal cord (C2-4 segment). The body of first thoracic vertebra was isointense in T1 and hyperintense on T2 sequences with contrast enhancement, suggestive of osteomyelitis. Cerebrospinal fluid (CSF) examination showed a cell count of 470 cells/ cmm (95% polymorphs and 5% lymphocytes), protein of 400 mg/ dL, and sugar of 55 mg/ dL. Gram stain and cultures were negative. Same day he developed breathlessness, his repeat X-ray chest showed increased bilateral lung infiltrates and blood gasses confirming the hypoxemia. Patient was transferred to the ICU and was connected to the ventilatory support. At this time an abscess was noted to point at the lower thoracic area, which was drained, yielding about one liter of yellowish pus, which was sent for the culture. Blood culture sent earlier grew MRSA sensitive to vancomycin. Subsequent cultures from nasal cavity, axilla, and groin did not show any bacterial growth. The antibiotic regimen was changed to vancomycin and continued for four weeks. Two days after drainage of pus and change of antibiotic, the patient started showing improvement. The pus also grew MRSA sensitive to vancomycin. The MRSA isolated from the pus and blood was subjected to molecular characterization. Staphylococcal cassette chromosome (SCCmec) typing was performed by a series of multiplex polymerase chain reactions (PCRs) to determine the mec and cassette chromosome recombinase (ccr) complexes. [2] Isolates from both the specimen were positive for type V SCCmec cassette and carried ccrC recombinase and mec C2-complex that are characteristics of type V cassette. CA-MRSA typically harbors SCCmec type IV or V cassettes. Both specimens were positive by PCR for Panton-Valentine Leucocidin (PVL) gene, whose production has been epidemiologically linked to particular Staphylococcus aureus infections including skin and soft tissue, severe necrotizing pneumonia, and bone and joint infections. [3] Both pus and blood isolates were positive for staphylococcal entero-toxin A (sea) with the blood isolate carrying sed in addition to sea. [4] Staphylococcal protein A (spa) typing of the blood isolate was carried out and the spa type from the repeat sequences was t657 (assigned from the Ridom data base). [5] The allelic patterns obtained from multi-locus sequence typing (MLST) of other isolates with the same spa type (t657), assigned a sequence type (ST) of 772 to the blood isolate. [6] ST772 is a single locus variant of ST1 and has been reported from Bangladesh, Netherlands, Norway, and Portugal. ST1 itself is present in many other countries including the United States. This is the first disease isolate belonging to SCCmec type V and ST772, causing pyomyositis, from India. The pulsed field gel electrophoresis (PFGE) pattern of this isolate was related to other ST772 isolates from nasal swabs of healthy people that we have characterized (data not shown). Majority of type V isolates have been reported in a ST59 background from Taiwan and this is the first report of SCCmec type V CA-MRSA in a ST772 genetic background. This is the first reported disease isolate belonging to SCCmec type V and ST772, causing pyomyositis, from India. The patient was discharged from the hospital after a stay of six weeks with no deficits and he was asymptomatic during his follow-up visit two months later. Discussion Our patient had interesting features like pyomyositis involving the paraspinal muscles, myelitis, bronchopneumonia, spinal osteomyelitis, isolation of MRSA from both blood and pus, and complete recovery with antibiotics and surgical drainage of the pus. We thought the muscle involvement is unlikely to be secondary to spinal osteomyelitis because of the extensive cervical and thoracic paraspinal muscle involvement compared to the single vertebral involvement by the osteomyelitis (MRI), history of exertion prior to the onset of illness and nature of his presenting symptoms. The myelitis, arachnoiditis, osteomyelitis, and pneumonia may be due to simultaneous involvement of these sites during bacteremia. Primary pyomyositis is believed to be due to transient bacteremia, and skeletal muscles are resistant to bacterial infections under normal circumstances. In patients who had died of staphylococcal septicemia, less than one percent of the cases had muscle involvement. [7] Therefore, predisposing factors are likely to be present which will aid in the pathogenesis of muscle infection. In our patient vigorous physical exertion could have predisposed the patient for developing pyomyositis. Our patient presented with invasive stage, followed by suppurative and septic stages. In pyomyositis, paraspinal muscles are affected in only 3.8% of cases. [8] Diagnosis depends on high index of clinical suspicion. Management includes both medical treatment with parenteral antibiotics covering Staphylococcus aureus and surgical drainage of the abscess. [1] Our patient had only paraspinal muscle involvement, but the presence of localized pain, redness and warmth gave a clue to the diagnosis clinically and MRI confirmed it. We should have started parenteral cloxacillin or oxacillin from the beginning because 95% of staphylococci are resistant to penicillin. [9] Friess and Wasenko have earlier reported a case of staphylococcal myelitis with successful treatment by antibiotic therapy, [10] but there was no associated pyomysitis. Our patient also had clinical features of cervical myelitis confirmed by the MRI findings with associated pyomyositis. Over the past few years, infections caused by CA-MRSA have become commonplace in United States and worldwide, and at one center, 62% of CA-Staphylococus aureus infections were due to MRSA. [11] A case of CA-MRSA is defined as illness compatible with staphylococcal disease in a patient residing in the community and isolation of the organism from clinically relevant site. [12] Our patient satisfied the above criteria. The first case report of MRSA pyomyositis in the literature is from Singapore in 1996. [13] There have been increasing reports of CA-MRSA emerging as an important cause of pyomyositis. [14] There are no reports of CA-MRSA pyomyositis from India, but in a recent study of nasal carriage of Staphylococcus aureus from India 18% of the isolates from the community were resistant to oxacillin, [15] and 11% of community-acquired pyoderma caused by Staphylococcus aureus isolates were resistant to methicillin. [16] In summary, to our knowledge this is the first case report of CA-MRSA pyomyositis from India, caused by a PVL positive isolate belonging to type V SCCmec and in a ST772 genetic background, showcasing varied manifestations of the staphylococcal infection. It also raises a question whether vancomycin should be considered in the critically ill community-acquired staphylococcal infections. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09182f1.jpg] [ni09182f2.jpg] |
| |||||||||

{kind=link}
{kind=link}