 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 57, No. 5, September-October, 2009, pp. 661-668 Case Report Intraspinal primitive neuroectodermal tumors: Report of four cases and review of the literature Jingyu Chen, Jinning Song, Hui Meng, Hua Feng Department of Neurosurgery, Southwest Hospital, Third Military Medical University, Chongqing - 400 038, The People's Republic of China Date of Acceptance: 02-Jul-2009 Code Number: ni09185 PMID: 19934573 DOI: 10.4103/0028-3886.57804
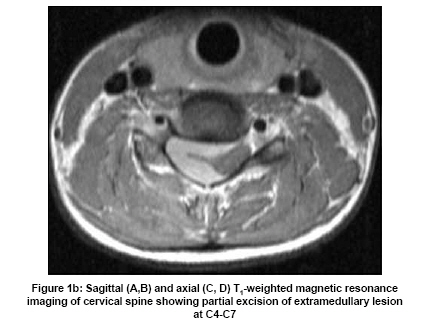
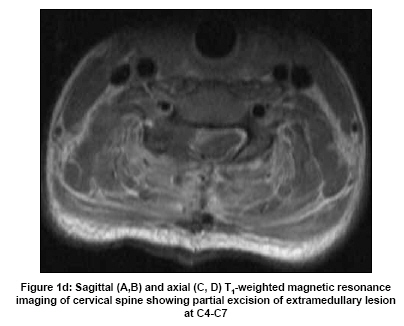
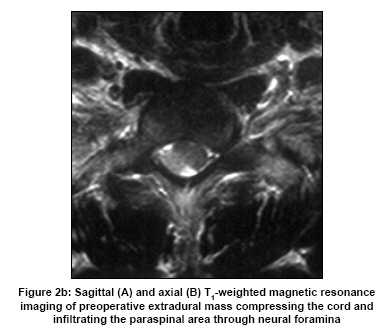
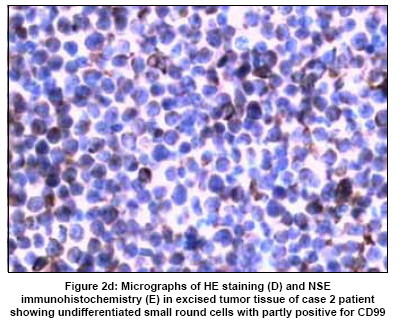
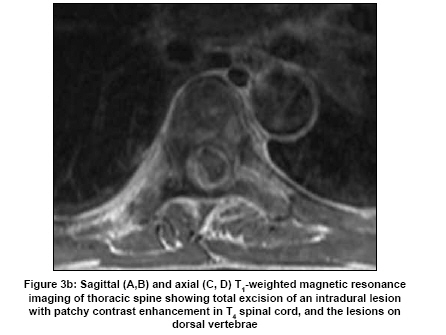
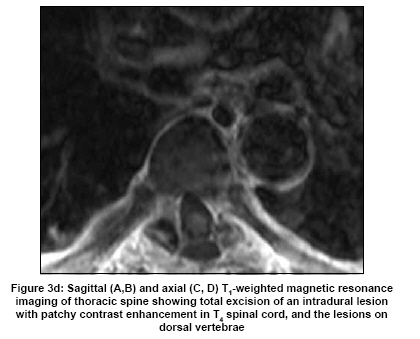
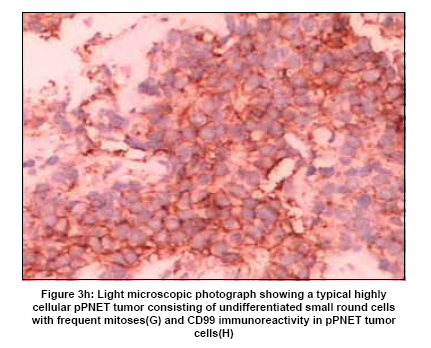
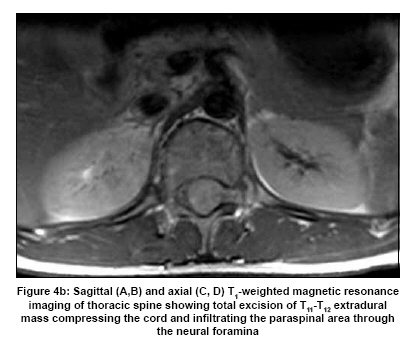
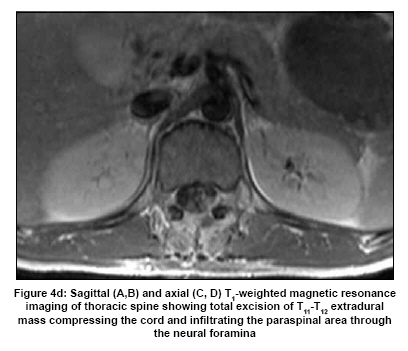
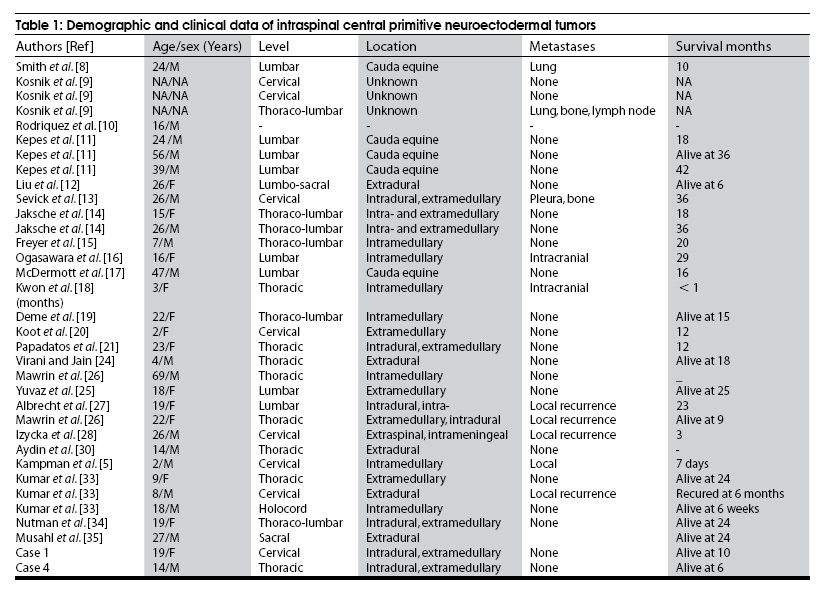
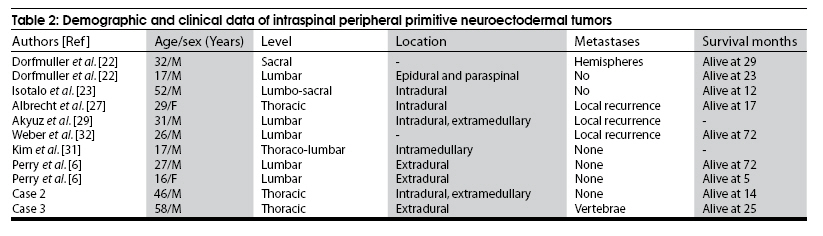
Abstract Intraspinal primitive neuroectodermal tumors (PNETs) are extremely rare and are aggressive with poor outcomes. Till date only 41 cases of intraspinal PNET have been reported. Here we report four new cases. Total excision of the tumor was done in three patients and partial excision in one patient. The unusual clinical features were vertebral metasis in one patient and short history of symptoms for four dasy. All had surgical excision, total excision in three patients and gross partial excision in one patient. Three patients were treated with craniospinal radiotherapy and chemotherapy. All the four patients are alive and asymptomatic at 6 to 25 months of followup.Keywords: Chemotherapy, neurosurgery, primitive neuroectodermal tumor, spinal cord, radiotherapy Introduction As for the World Health Organization (WHO) classification of brain tumors, [1] all undifferentiated (primitive) tumors are derived from common neuroepithelial cells and are thus classified under primitive neuroectodermal tumors (PNET). The undifferentiated or poorly differentiated neuroepithelial cells have the multipotent capability of differentiating into divergent lineages including neurons, astrocytes, ependymal cells, muscle cells or melanocytes. Hart and Earle were the first to introduce the term PENT in 1973, [2] These tumors are more common in children. There is considerable confusion and controversy in the classification of PNETs. [3] Central PNETs (cPNET) develop from the central nervous system (CNS) and peripheral PNETs (pPNET) putatively from the neural crest. [4] This confusion may partly be due to overlap of CNS and peripheral nervous system at the spinal level. [5],[6] Both cPNET and pPNET, are aggressive tumors and have similar survival rates. However they differ in their clinical presentation and spread pattern. [5] They also have distinct immunohistochemical profiles and clinical evolution and treatment protocols also differ. PNETs are mainly intracranial, predominantly in the cerebellum. [7] Intraspinal PNETs are extremely rare. Only 41 cases have been reported in the literature till date. [5],[6],[8],[9],[10],[11],[12],[13],[14],[15],[16],[17],[18],[19],[20],[21],[22],[23],[24],[25],[26],[27],[28],[29],[30],[31],[32],[33],[34],[35] In this communication we report four cases of intraspinal PNET and also review literature on intraspinal PNET. Case Reports Case 1 A 19-year-old woman presented with right side neck pain and progressive weakness of all the four limbs of 45 days duration. She was bedridden five days before the admission. On examination, the motor power was grade 1/5 in the right upper limb and grade 2-3/5 in the remaining limbs. Magnetic resonance imaging (MRI) of the cervical spine revealed an extramedullary lesion extending from C 4 to C 7 vertebral level on the right side. The lesion was isointensity on T1-weighted image and hyperintensity on T2-weighted image [Figure - 1a] and b. A provisional diagnosis of spinal meningioma was made. Through a C 4 -to-C 7 laminectomy, a gross partial excision of the lesion was achieved [Figure - 1c] and d. The tumor was soft, mauve, vascular and completely extramedullary in location, encasing a nerve root. Histopathological examination and immunohistochemical staining confirmed the diagnosis of PNET. By the third postoperative week, the patient was ambulatory without support. She had six cycles of chemothotherapy consisting of cyclophosphamide and temozolomide, followed by cranio-spinal radiation therapy spread over eight weeks. She was alive at ten months postoperatively. Case 2 A 46-year-old man presented with a four-day history of progressive weakness of the lower limbs and urinary retention. On neurological examination, motor power was grade 3/5 in the lower limbs, tendon reflexes were brisk and both the plantars were upgoing. He had hypoesthesia below T 4 level. MRI of thoracic spine showed an intradural extramedullary tumor at the T 1 -T 2 level compressing the cord [Figure - 2a] and b. Preoperative cranial MRI and thorax and abdomen computerized tomography (CT) were negative for any tumor pathology. A laminectomy was performed at the T 1 -T 2 vertebrae levels. At exploration, the intradural mass was subpial, soft grayish, adherent to the the spinal cord and encasing the nerve roots. A total excision was achieved. Postoperatively he had a partial improvement in the deficits. Histopathology and immunohistochemistry of the lesion revealed PNET [Figure - 2c] and d. He received chemotherapy consisting of vincristine, cyclophosphamide, and doxorubicin and also focal radiation therapy spread over a period of four weeks. There was no progression of the disease at the end of 14 months post-surgery. Case 3 A 58-year-old man presented with thoracic back pain of three months duration and progressive weakness of the lower limbs of 15 days duration. On neurological examination, motor power was grade 0/5 in the lower limbs, tendon reflexes were pathological and both the plantars were upgoing. He had hypoesthesia below T 3 level. MRI of the thoracic spine revealed a posterior intraspinal epidural lesion at the T 4 level compressing the cord and several lesions in the body of the thorax vertebrae [Figure - 3a] and b. Positron emitted tomography-computed tomography (PET-CT) of whole body showed metastasis to vertebrae [Figure - 3f]. A laminectomy was performed from T 1 to T 2 and an epidurally located, capsulated mass, gray in color and without any adherence to the adjacent structures was totally excised [Figure - 3c] and d. The diagnosis of PNET was confirmed by histopathological and immunohistochemical examination [Figure - 3g] and h. During the early postoperative course, he had rapid neurological recovery and was able to walk unassisted. He did not receive any adjuvant therapy due to socioeconomic issues. He was alive at 25 months and remained alive in the 25 th month after operation. Case 4 A 14-year-old boy presented with back pain and progressive weakness of both the lower limbs of four months duration. The patient had become bedridden for seven days and had been urine and stool incontinent for six days. On physical examination, power in the lower limbs was grade 1/5, and there was a hypoesthesia below T 8 level. MRI showed an intradural extramedullary tumor at T 11 -T 12 level compressing the cord. Through a T 11 -T 12 laminectomy, an intradural extramedullary vascular lesion was noted encasing the nerve roots and conus [Figure - 4a] and b. At exploration, the intradural mass was subpial, soft and grayish. The mass was totally excised [Figure - 4c] and d. Histopathology confirmed PNET. After surgical recovery, the patient received the same dose of radiotherapy and chemotherapy like in case 1.The patient was able to walk unassisted at six months of follow-up. Discussion Intraspinal PNET is extremely rare. Recently in 2006 Kampman et al., had reviewed the clinical characters and genetics of 28 cases of intraspinal PNET reported in the literature. [5] Since then 13 additional cases of intraspinal PNET have been reported. However, the histopathologic distinction between cPNET and pPNET has not been made in most of the reported cases. Kampman et al., [5] had recently summarized the distinguishing features between cPNET and pPNET. We summarized the clinical characteristics of the 45 cases, including our four cases, of intraspinal PNET reported till date in [Table - 1] and [Table - 2]. Intraspinal PNET has adult onset and male predominance. The average age at presentation for patients with intraspinal PNET was 24.1 years (range three months to 69 years) much higher than the average age for intracranial PNET, [7] The duration of illness is often short, less than four months and it can be as short as four day seen in one (Case 2) of our patients. These tumors can occur at any levels of the spine and the location can be intramedullarily, intradural-extramedullarily or epidurally. Only 12 cases of pPNET with positive immunostaining for CD99 or PGP 9.5, have been reported and half of them were in the lumbar region. This might be due to the fact that the cauda equina forms part of the peripheral nervous system. Cranial symptoms are not a feature of primary intraspinal PNET. This is a feature that distinguishes primary intraspinal PNET from primary intracranial PNET with spinal metastasis. All our patients underwent cranial imaging postoperatively with no evidence of any pathology [Figure - 1e],[Figure - 2e],[Figure - 3e] and [Figure - 4e]. MRI features are not specific for this lesion as was seen in our four cases. The cPNET frequently disseminates via the cerebrospinal fluid and rarely metastasize out side the CNS, and pPNET may disseminate to distant sites. However, intraspinal PNET is locally aggressive and local recurrences are common. Of the 33 patients with primary intraspinal cPNET [Table - 1], 10 patients had metastasized to distant sites: Leptomeninges in two, lymph node in two, lung in two, pleura in one, and intracranial in 3. Of the 12 patients with pPNET [Table - 2], only one patient had metastazed to the cerebral hemisphere and we report the first case with distant vertebral metastasis (Case 3). In all the reported cases the diagnosis was established by histopathology and immunohistochemistry. The characteristics diagnostic features of PNET by histopathology and immunohistochemistry include: (1) poorly differentiated small, round/spindle-shaped cells [Figure - 3g]; (2) densely packed or in sheets or nests; (3) positive for neuronal or glial markers like neuron-specific enolase, CD99, synaptophysin, glial fibrillary acidic protein (GFAP), S-100, etc., Recent studies suggest that the expression of MIC2 glycoprotein by immunocytochemical staining (CD99) can help to differentiate between central and peripheral PNET. [5] Similarly in situ hybridization analysis of mRNA expression for specific genes can be used to diagnose the PNET subtypes and plan optimal treatment protocol. [36] In view of the limited number of reported cases, the optimal treatment for intraspinal PNET has not yet been defined. Surgical excession and decompression is the primary mode of treatment. Neurologic empovement is often noted in most of the patients following surgery. Craniospinal irradiation and hyperfractionated radiotherapy of the tumor region have been shown to be of benefit. [22] Though there is no agreement on the chemotherapy regimens, successful results have been reported using combinations of cyclophosphamide or ifosfamide, cisplatin or carboplatin, and vincristine-peplomycin. [19] The chemotherapy protocol for cPNET should be different from that for pPNET, as the latter is more closely related to Ewing's sarcoma. Peripheral blood stem cell transfusion for PNET has been recently proposed. [37] Three of our patients were treated with postoperative radiotherapy and chemotherapy, and all our patients are still alive and asymptomatic for 6-25 months. Despite the aggressive treatment with adjuvant radiotherapy and chemotherapy, most of the patients die within three years (range: 3 months-72 months). There is still a need for more clinical studies to explore reasonable strategies of treatment. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09185f2c.jpg] [ni09185f4a.jpg] [ni09185f3d.jpg] [ni09185f1c.jpg] [ni09185f2d.jpg] [ni09185t2.jpg] [ni09185f1e.jpg] [ni09185f2b.jpg] [ni09185f1d.jpg] [ni09185f3h.jpg] [ni09185f2e.jpg] [ni09185f3f.jpg] [ni09185f4b.jpg] [ni09185f2a.jpg] [ni09185f4c.jpg] [ni09185f1a.jpg] [ni09185f3a.jpg] [ni09185f3b.jpg] [ni09185f1b.jpg] [ni09185f3g.jpg] [ni09185f3c.jpg] [ni09185t1.jpg] [ni09185f4e.jpg] [ni09185f4d.jpg] [ni09185f3e.jpg] |
| |||||||||


![Figure - 1a]](/showimage?ni/photo/ni09185f1a.jpg){kind=link}
{kind=link}
![Figure - 1c]](/showimage?ni/photo/ni09185f1c.jpg){kind=link}
{kind=link}
![Figure - 2a]](/showimage?ni/photo/ni09185f2a.jpg){kind=link}
{kind=link}
![Figure - 2c]](/showimage?ni/photo/ni09185f2c.jpg){kind=link}
{kind=link}
![Figure - 3a]](/showimage?ni/photo/ni09185f3a.jpg){kind=link}
{kind=link}
![Figure - 3f]](/showimage?ni/photo/ni09185f3f.jpg){kind=link}
![Figure - 3c]](/showimage?ni/photo/ni09185f3c.jpg){kind=link}
{kind=link}
![Figure - 3g]](/showimage?ni/photo/ni09185f3g.jpg){kind=link}
{kind=link}
![Figure - 4a]](/showimage?ni/photo/ni09185f4a.jpg){kind=link}
{kind=link}
![Figure - 4c]](/showimage?ni/photo/ni09185f4c.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
![Figure - 1e]](/showimage?ni/photo/ni09185f1e.jpg){kind=link}
![Figure - 2e]](/showimage?ni/photo/ni09185f2e.jpg){kind=link}
![Figure - 3e]](/showimage?ni/photo/ni09185f3e.jpg){kind=link}
![Figure - 4e]](/showimage?ni/photo/ni09185f4e.jpg){kind=link}