 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
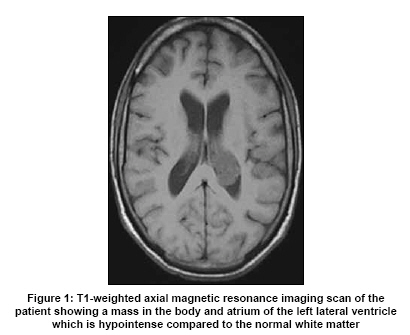
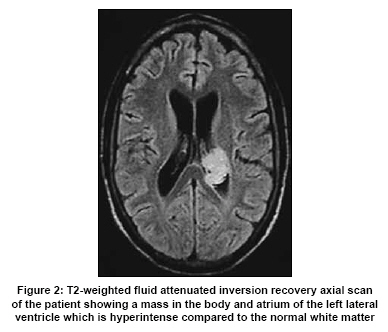
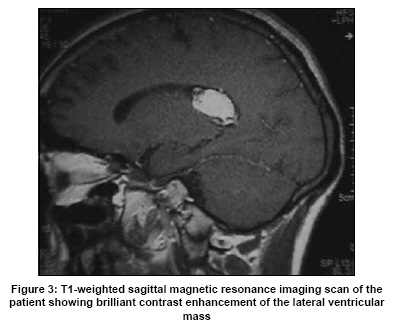
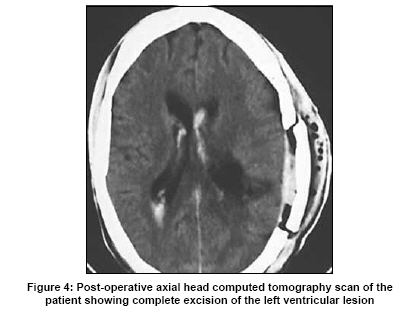
Neurology India, Vol. 57, No. 5, September-October, 2009, pp. 677-679 Letter To Editor Hemangioblastoma of the lateral ventricle Ramandeep Singh Jaggi, Ishwar Chandra Premsagar, Abhishek Department of Neurosurgery, Dr. R.M.L. Hospital, Baba Kharak Singh Marg, New Delhi - 110 001 Date of Acceptance: 10-Feb-2009 Code Number: ni09191 PMID: 19934579 DOI: 10.4103/0028-3886.57797 Sir, Hemangioblastomas are the most frequent vascular tumor of the central nervous system (CNS) [1] and can be associated with von Hippel-Lindau (VHL) disease in 3 to 38% of the cases as a major manifestation. [2] These tumors are predominantly found in the cerebellum, spinal cord, and brainstem. [2] The unusual locations include leptomeninges and sellar-sphenoid sinus. [4],[5],[6] Supratentorial location accounts for 4 to13% of the cases. [2] However, hemangioblastomas of the lateral ventricle are extremely rare and only 5 cases have been reported in the English literature till 2001. [2] We report a unique case of a lateral ventricular hemangioblastoma. A 30-year-old male presented with a progressive holocranial headache of six months duration. The neurological examination was normal. Magnetic resonance imaging (MRI) of the brain showed a 3 x 2 cm mass in the left lateral ventricle, which was hypointense on T1-weighted images, hyperintense on T2-weighted as well as fl uid attenuated inversion recovery (FLAIR) images. The tumor showed brilliant contrast enhancement [Figure - 1],[Figure - 2],[Figure - 3]. The patient had a left-sided parietal craniotomy and through a trans-sulcal approach through the superior parietal lobule the lesion was excised. At operation the lesion was brownish red, soft to firm, highly vascular, and was adherent to the ventricular ependyma as well as the choroid plexus. An immediate post-operative computed tomography (CT) scan showed complete excision of lesion [Figure - 4]. Post-operatively, the patient had transient sensory aphasia, which recovered fully in a 1 month. A histopathological examination showed tissue composed of a fi ne network of blood spaces separated by numerous polygonal stromal cells, with lighty stained cytoplasm [Figure - 5]. Immunohistochemical staining showed a strong immunopositivity in several stromal cells for vimentin, epithelial membrane antigen (EMA), and neuron specifi c enolase (NSE) - typical of a hemangioblastoma. The patient was investigated for other features of von Hippel-Lindau syndrome but none were found. Hemangioblastomas of the CNS are infrequent and they account for 2% of primary CNS tumors. [1],[3] The most common location is the posterior fossa, cerebellar hemisphere accounting for 83%. [3] Supratentorial location is rare, sporadic hemangioblastomas 4% and VHL disease 13%. [2] The lateral ventricular location is extremely unusual, only four symptomatic cases [7],[8],[9],[10] and one incidental postmortem finding [8] have been described. All the four lateral ventricle hemangioblastomas reported till date had been in patients with VHL disease. [7],[8],[9],[10] In our patient we could not find any evidence for VHL disease. However, it is prudent to investigate patients with lateral ventricular hemangioblastoma for VHL disease. The size of the lateral ventricle hemangioblastomas in all the four documented cases has been greater than the size of the hemangioblastoma in other locations. This may partly be related to the fact that the volume of the lateral ventricle can accommodate a reasonable size mass lesion and any mass lesion in the lateral ventricle has to grow to a sufficient size to produce symptoms. In other locations cystic component of hemangioblastoma has been the contributing factor to the size of the tumor, whereas all the lateral ventricle hemangioblastomas including our case were solid. [7],[8],[9],[10] Hemangioblastoma of the lateral ventricle is associated with a better prognosis than its counterpart in the third ventricle. Diehl and Symon were able to achieve complete resection of the tumor. [11] Our experience was also similar. We were able to achieve good control of the feeding vessels from the choroids plexus and the wall of the lateral ventricle, thus enabling in toto resection of the tumor. Post-operative dysphasia/mutism is an infrequent and usually transient complication of hemangioblastoma surgery. In our case, it was probably related to the proximity of the tumor to the posterolateral region of the thalamus and/or surgeryrelated edema and/or ischemia in the parietal region. Its incidence can be reduced by delineating the speech area by functional MRI preoperatively [12] or by using intraoperative cortical mapping. [13] References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09191f2.jpg] [ni09191f4.jpg] [ni09191f1.jpg] [ni09191f5.jpg] [ni09191f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}