 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
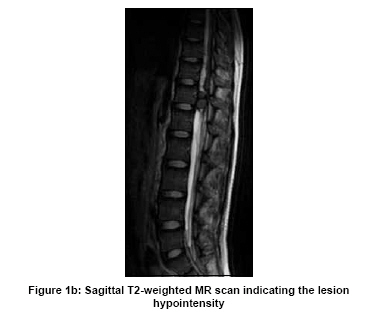
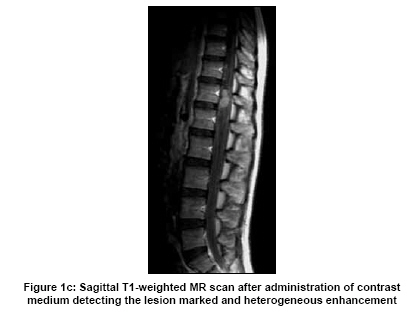
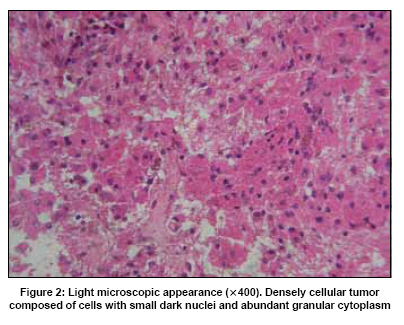
Neurology India, Vol. 57, No. 5, September-October, 2009, pp. 679-681 Letter To Editor Subdural granular cell tumor in thoracic vertebral canal Jinrong Qu, Jun Ma, Lin Luo1 , Lin Ai, Shaowu Li, Jianping Dai Departments of Neuroradiology and 1 Pathology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China. Date of Acceptance: 06-Feb-2009 Code Number: ni09192 PMID: 19934580 DOI: 10.4103/0028-3886.57799 Sir, Granular cell tumors have been reported in different locations such as skin, subcutaneous tissue, gastrointestinal tract, and intrathoracic. [1] However, spinal location was extremely rare, only two cases of spinal intradural location granular cell tumors were document since the first description in this location in 1926. [2],[3] We report a patient with intraspinal granular cell tumor with detailed MRI findings. A 16-year girl presented with progressive back, thoraco- lumbar, pain of 40 days duration. Following lumber puncture, she developed increased numbness, weakness, and paraesthesia in both the lower limbs. She had good health before this illness. Neurologic examination showed decreased superficial sensations in both the lower limbs below first lumbar dermatome and the motor power was graded at 4/5. Magnetic resonance imaging (MRI) of the spine was performed with a 3.0T scanner, The MRI sequences studied included saggital T1-weighted (TR 600 ms, TE 12 ms slice thickness 4 mm), turbo spin-echo T2-weighted (TR 3800 ms, TE 113 ms, slice thickness 4 mm) and axial T2-weighted (TR 3850 ms, TE 106 ms, slice thickness 8 mm) sequence without fat saturation. A T1-weighted axial, sagittal, and coronal scan were repeated after intravenous administration of paramagnetic contrast media. The MRI showed an irregular 10 x 21 x 7 mm 3 mass located in the subdural space at the T11-T12 level. The lesion was isointense on T1-weighted images and was hypointense on T2-weighted images. No peri-lesional edema was seen in the adjacent marrow. The neighboring marrow was compressed without an abnormal signal. On post- contrast imaging, it showed markedly heterogeneous enhancement [Figure - 1]a, b, c. During the operation, the tumor revealed a single nodule and was sharply-edged in the subarachnoid space. It was conglutinated with the coccygeal nerve and arachnoid membrane. It was fragile in consistency and yellow in color with moderate blood supply. Light microscopy features: Densely cellular tumor composed of cells with small dark nuclei and abundant granular cytoplasm. Special stain indicated that CD68, Vimentin, and NSE were positive, and Chromogranin was negative [Figure - 2]. Granular cell tumors in the central nervous system (CNS) was reported in the spinal intradural location [2],[3] and in the neurohypophysis and pituitary stalk, about 50 cases since the first documentation in 1893. [4] The cell of origin is controversial. Some investigators suggested that CNS granular cell tumors derive from schwann cells, however, others insisted that the cell of origin for neurohypophyseal granular cell tumors is the pituicyte, which is a modified astrocyte. [4],[5],[6],[7],[8],[9] Lee et al., suggested that granular cell tumors derive not only from schwann cells but also degenerated normal cells and tumor cells. [10] The growth characteristics of granular cell tumors outside of the CNS are variable. Most reports have emphasized their benign nature while several others have described it as a malignant form. The histochemical and ultrastructural features of a metastasizing malignant granular cell tumor [11] were similar to those of the benign granular cell tumors. In our patient the tumor characteristics were benign, had a sharp margin and was confined to leptomeninges (subarachnoid space) and did not significantly distort or compress the underlying spinal cord. There was minimal extension into the pia and external glial membrane. There were no significantly neurologic deficits. The light microscopic characteristics of the cells in both the previously described intradural spinal granular cell tumors were similar to the findings described in the granular cell tumors in other locations. The voluminous cytoplasm contained abundant PAS-positive granules. [2],[3] Because granular cell tumor tissue is compact and dense, the tumor would be isointense on T1WI and hypointense on T2WI. On post-contrast imaging, the lesion shows moderate or remark enhancement. Granular cell tumor in the subdural space should be differentiated from meningioma and schwannoma. In the absence of calcification, it is difficult to distinguish meningioma from a granular cell tumor. Typical features of the nerve sheath tumor is a dumbbell-shaped lesion with both intraforaminal and extraforaminal components. However, when nerve sheath tumors shows a solitary lesion, it is also impossible to be distinguished from a granular cell tumor. There have been case reports of granular cell tumors occurring during pregnancy and hyperestrogenic states. [12],[13] Our patient was a girl, however we had not done estrogen levels in her. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09192f1c.jpg] [ni09192f1b.jpg] [ni09192f2.jpg] [ni09192f1a.jpg] |
| |||||||||

![Figure - 1]a](/showimage?ni/photo/ni09192f1a.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}