 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
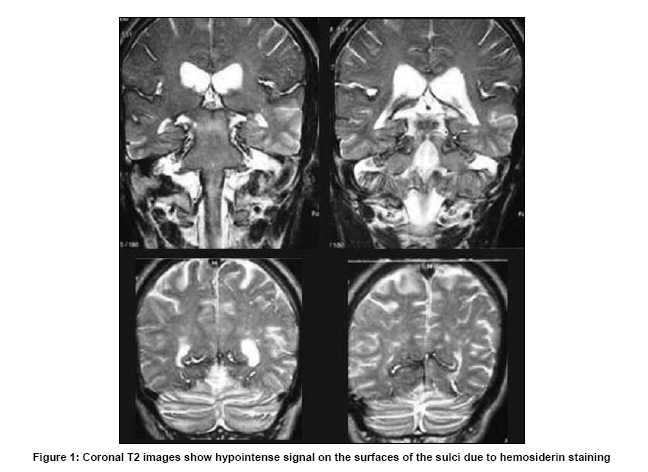
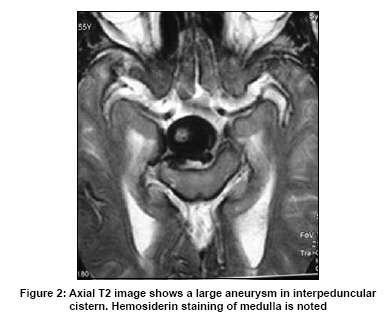
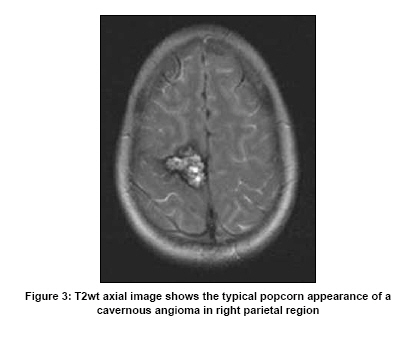
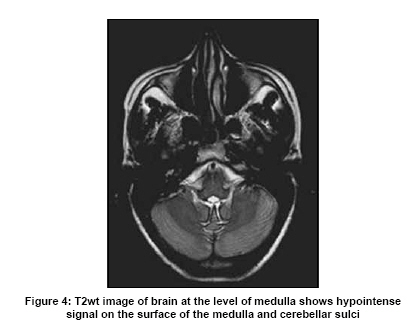
Neurology India, Vol. 57, No. 5, September-October, 2009, pp. 687-688 Neuroimage Superficial siderosis Naseer A. Choh, Omar S. Kirmani , Suhil Choh1 , Majid Jehangir Departments of Radiology, and 1 Pediatrics, SMHS Hospital, Srinagar, SKIMS, Soura, India Date of Acceptance: 12-Aug-2009 Code Number: ni09196 PMID: 19934584 DOI: 10.4103/0028-3886.57785 Case 1 An elderly patient presented with insidious onset of sensorineural hearing loss. The past history was unremarkable except for insidious onset of weakness of left lower limb. Physical examination revealed left hemiparesis with upgoing left plantar. Magnetic resonance imaging (MRI) of brain revealed a large flow void in the interpeduncular cistern suggestive of aneurysm arising from the top of the basilar artery. In addition, hypointense signal was noted (prominent on T2 and FLAIR images) on the surface of both cerebral hemispheres, the pons, cerebellar folia and medulla. The final diagnosis was superficial siderosis secondary to leaking basilar artery aneurysm [Figure - 1] and [Figure - 2]. Case 2 A middle-aged female, with complaints of progressive ataxia and bilateral sensorineural hearing loss was referred for MRI of brain. The patient had significant medical history of adult onset seizure disorder well controlled with anti-epileptic drugs. Physical examination revealed senorineural deafness and limb and gait ataxia. Computed tomography (CT) showed a small intraparenchymal hyperdense lesion in the right parietal region suggestive of hematoma. MRI of brain revealed a typical popcorn lesion in right parietal region with heterogeneous signal intensity on T1, T2 and FLAIR images with fluid levels suggestive of a cavernous angioma. In addition, hypointense signal was noted (especially on T2 images) coating the cerebral sulci, pons, midbrain and medulla. Mild cerebellar cortical atrophy was also noted [Figure - 3] and [Figure - 4]. The final diagnosis was superficial siderosis secondary to cavernous malformation. Superficial siderosis is the result of chronic and recurrent subarachnoid hemorrhage and the causes include: Postoperative cerebrospinal fluid cavity, cerebral aneurysms, vascular malformations, cervical root avulsion, hemorrhagic neoplasms, etc. CT is insensitive in detecting siderosis, but may reveal cerebral and cerebellar cortical atrophy that is associated with superficial siderosis. [1],[2],[3] The MR findings are dramatic, with the brain surface and cranial nerves outlined by a profound hypointense signal on T2 MR images. T2 gradient echo (GRE) images are very sensitive to hemosiderin deposition and show blooming of the hypointense signal. [4] The source of recurrent bleed may sometimes be located in the spine which should always be screened if no cause is found by imaging of brain. [1],[2] It is a rare progressive disorder with a prevalence of 0.15% in patients undergoing MRI. However, recent studies have reported a prevalence of 0.7% in the elderly without dementia and it has been attributed to micobleeds. [5] Hemosiderin is a neurotoxic agent that is responsible for neuronal and glial damage resulting especially in eighth cranial nerve damage and cerebellar atrophy that account for the characteristic clinical features of this disorder. The most common clinical manifestationsinclude bilateral sensorineural hearing loss (SNHL) (95%) and ataxia (88%). [6],[7] The other features include bilateral hemiparesis, bladderdisturbances, anosmia, dementia and headache. [1],[2] The treatment is directed at the underlying cause; cochlear transplantation may be required for SNHL. [2] References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09196f4.jpg] [ni09196f2.jpg] [ni09196f1.jpg] [ni09196f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}