 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
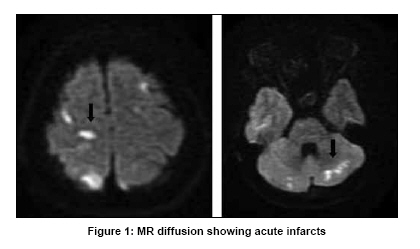
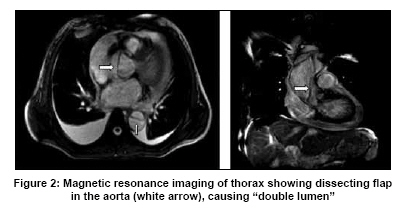
Neurology India, Vol. 57, No. 5, September-October, 2009, pp. 689 Neuroimage Aortic dissection causing embolic stroke E. Fernandez, Raghunandhan Nadig, Thomas Mathew, G. R. K. Sarma Department of Neurology, St. Johns Medical College and Hospital, Bangalore - 560 034, India Date of Acceptance: 02-Jul-2009 Code Number: ni09197 PMID: 19934585 DOI: 10.4103/0028-3886.57784 A 45-year-old female, known hypertensive for the past five years, presented with an episode of generalized seizure. She also had diffuse headache and mild retrosternal chest pain just few hours prior to the episode of unconsciousness. On examination, pulse was 68 min, normal rhythm, volume, character, and all peripheral pulses were well felt and blood pressure was 170/100 mmHg. Cardiac auscultation revealed early diastolic murmur in the right parasternal area. On neurological examination the deep tendon reflexes were exaggerated and plantar were bilaterally flexor, and tandem gait was ataxic. Diffusion-weighted magnetic resonance imaging (MRI) of brain revealed multiple small hyperintense lesions involving bilateral subcortical areas and cerebellar white matter, suggesting acute embolic infarcts [Figure - 1]. Transthoracic echo cardiogram revealed dilated ascending aorta and an intimal flap suggestive of dissection. MR aortogram confirmed the same, the dissection extending from ascending aorta till bifurcation of aorta [Figure - 2]. Her carotid and vertebral arteries were normal. Aortic dissection is a rare and potentially fatal disease, with an estimated incidence of 5-30 cases per million per year. [1] Classically, aortic dissection presents with sudden and severe pain in the chest, back, or abdomen. Patients often describe tearing or ripping pain radiating to the interscapular region. There are a few reports of atypical findings or no pain in the literature. Cerebral ischemic complications occur in 18-30% of aortic dissections. [2] They result from occlusion of the origin of the common carotid by dissection flap or due to artery-to-artery embolism from a thrombus developed on the intimal surface of the dissected artery. [3] Chronic systemic hypertension is the most common risk factor, followed by connective tissue diseases such as Marfans syndrome and Ehlers Danlos syndrome. [4] Our patient had no clinical signs of connective tissue disease. One unique finding in this patient was the presence of normal peripheral pulses. The diagnosis was made by a combination of clinical suspicion, echocardiography, and MR aortogram. Aortic dissection has varied presentations and requires a high degree of clinical suspicion for an early and accurate diagnosis. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09197f1.jpg] [ni09197f2.jpg] |
| |||||||||

{kind=link}
{kind=link}