 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
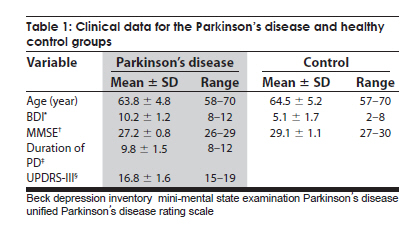
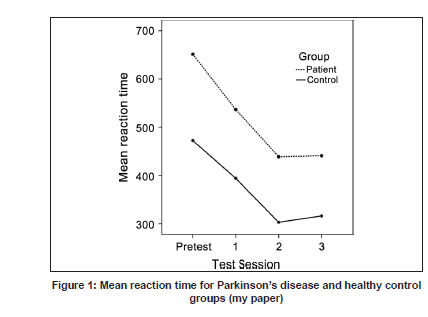
Neurology India, Vol. 57, No. 6, November-December, 2009, pp. 768-771 Brief Report Effects of motor skill practice on reaction time and learning retention in Parkinson's disease Hamid Reza Rostami 1 , Hassan Ashayeri Department of Occupational Therapy, Faculty of Rehabilitation, Ahwaz Jundi Shapour University of Medical Sciences, Ahwaz, Date of Acceptance: 30-Nov-2009 Code Number: ni09214 PMID: 20139507 DOI: 10.4103/0028-3886.59474 Abstract One of the prominent disturbances in Parkinson's disease (PD) is bradykinesia. We studied performance of hand-to-mouth reach reaction time (RT) in right-handed PD patients and nine age and sex matched healthy control subjects. Participants practiced hand-to-mouth reach skill in response to a visual stimulus, 120 times a day for a period of one week. Using Kinemetrix 3D Motion Analysis system, the effects of motor skill practice and learning retention were investigated. Pretest performance was compared with performances on the second and seventh day of the study, and also performance on fourteenth day with no further practice for one week. There was a significant reduction in the mean RT in the control group after one week of practice. In PD patients the reduction in the mean RT was significant between pretest and first test sessions (P < 0.01). However, the difference was not significant between the first and second session (P = 0.06) and also between the second and third test sessions (P = 1.0). Short-term practice can improve bradykinesia in patients with PD but it is not long-lasting.Keywords: Bradykinesia, learning retention, Parkinson's disease, practice, reaction time Introduction Long-lasting improvement in performing skilled motor movements can be achieved by training and retraining and repeated practicing. [1],[2],[3] The stages involved in information processing are stimulus identification, response selection, and response programming. Response programming is defined as transforming a selected, cognitive or abstract idea of a movement response into a code as executive commands for the task. [4] Impaired movement execution is one of the features of Parkinson's disease (PD) and these patients have poor response programming as compared to stimulus identification and response selection. [5] Bradykinesia as a result of a slowdown in the speed of information processing is a fundamental feature of PD and contributes significantly to the overall disease-related disability. [6] All the phases of voluntary movement execution are impaired by bradykinesia, [7] thus PD patients spend more time than normal subjects, not only in the initiation of voluntary movements, [4],[8],[9] but also in the execution of voluntary movements. [3],[10] Antiparkinsonism drug therapy ('on' period) decreases the time of initiation and execution of movements, though not fully. [11] Most studies investigating the effect of brief period, minutes or hours, of practice have shown that learning is either normal [4],[12],[13] or slightly impaired [14],[15],[16] in mild to moderate PD patients. Studies investigating the effect of prolonged practice, two weeks, had shown reduced benefit in PD. [3] Smiley-Oyen et al., [17] have shown if people with PD are given sufficient practice they can learn and both memory-based and content driven movement sequences. However, the effect of prolonged practice on reaction time (RT) has not been study, hence this study. Materials and Methods Nine PD patients (mean age: 63.8 ± 4.8 years; seven males and two females; stage II of Hoehn and Yahr disability rating scale [18] ), and nine age and gender-matched healthy control subjects (mean age: 64.5 ± 5.2 years; seven males and two females) participated in the study with an informed consent. All participants were right-handed and in all of them left arm was more bradykinetic (Unified Parkinson's disease Rating Scale (UPDRS-III) [18] ) and all the patients practiced the skills with the left hand only. The patient's disease-related motor impairment was assessed by the motor examination section of the UPDRS-III and the modified Hoehn and Yahr staging according to the UPDRS- V. [18] In addition all the participants in the study had mini-mental status examination (MMSE), [19] and beck depression inventory (BDI) [20] before the study and people with score $13 on BDI and #26 on MMSE scales were excluded from the study. All the PD patients continued to be on the medication which they were taking earlier and no modification in the drug dosages were done during the study period. Patients took test and practice sessions one hour after the drug dose while in 'on' period of medication. All subjects in the study had normal visual acuity and had no physical disability in the upper limbs that might interfere with the experimental tasks. Instrument Kinemetrix 3D Motion Analysis System (UK 1997, MIE) was used to record the movements in three-dimensional space. The system comprised three infrared ray cameras, which in this study, recorded the motion of three passive markers placed on the lateral aspect of the wrist, elbow, and shoulder joints. A real-time TV image-converting processor connected to the cameras had digitalized the analog data and reconstructed the x, y, and z equivalents of the markers motion. Movement and kinematics parameters were displayed on the monitor in a graphic form and raw data was also obtained from system in the form of ASCII file. Procedure After the primary clinical assessments and calibration of the system, participants were asked to sit on a fixed and adjustable-height chair during the test and practice sessions. The arm was beside the body (shoulder: External rotation, elbow: 15 degree of flexion, forearm: Supination). Three markers were positioned on the lateral aspect of the wrist, elbow, and shoulder joints. During the test and practice sessions, participants were asked to look at the monitor that was specified for them. Fourth marker (stimulus marker) covered was positioned on the wall behind the participants. The marker got displayed on the monitor whenever the cover over the marker was removed. The stimulus was presented randomly during the test and practice sessions. Participants were expected to carry out hand-to-mouth reach in response to the stimulus on the monitor. During the entire period of the test movement analysis was done every 15 sec in all the participants. Reaction time was defined as the time interval between the visual stimulus presentation and the initiation of movement. The moment registration of fourth marker or stimulus marker was based on position-time graph of the system and the moment of initiation of the movement was determined based on the angle-time graph. In angle-time graph, both angle between two lines and velocity-time were used to specify the movement initiation. In other words, time of position change as well as velocity increase was calculated. The tester demonstrated the task, manually guided the participants through movement pattern, and allowed two practice trials of movement pattern. In order to carry out the experiment, in each test session, three trials were performed and mean RT of three trials was recorded as the retention time of people. Participants performed the hand-to-mouth motor skill in response to visual stimulus similar to test conditions, 120 times each day for one-week in following order: Ten repeats followed by 30 seconds rest. The only extrinsic feedback was given to all participants before each trial of practice was asking the participants to do the movements with as much accurate and fast as possible. The testing schedule comprised pretest on first day or baseline session, followed by first and second test on second and seventh days of practice. At seventh day, the practice was paused and the third test was carried out on the fourteenth day, to investigate the learning retention. Statistics The data were analyzed by SPSS software (Version 15). One-way ANOVA was used for matching the groups by age and Mann-Whitney U test to compare BDI and MMSE scores between the groups. The RT data were analyzed by ANOVA Repeated Measurements (2 x 4) that group (normal and Parkinson disease subjects) determined as a between-factor and test session as a repeated measure factor. Post-hoc analysis was performed with the Tukey's honestly significant difference to compare means across groups. All tests were conducted with the alpha level set at 0.05. Results Analysis of the age data for groups by a one-way ANOVA revealed no significant difference between groups. [Table - 1] presents descriptive data for group comparisons. Mann-Whitney U test for comparing BDI and MMSE scores between groups showed a significant difference only for depression scores, indicating that the PD patients have higher scores than normal subjects (P < 0.05). Analysis of data relating to RT by Kolmogorov-smirnov Z revealed normal distribution of data. Data analysis revealed no significant interaction between factors group and session [F (3, 48) = 0.53, P = 0.67]. Analysis of group effect, showed a significant difference [F (1, 16) = 7.05, P = 0.02] indicating that RT of patients was higher than healthy control subjects. Mean RT at first test session decreased significantly ( P < 0.01) compared to pretest values and patients showed more decrease in mean RT values (115 ms vs. 78 ms). At second test session, mean RT values decreased compared to pretest and first test sessions for both the groups but this was significant only in normal group. In PD patients, mean RT significantly reduced between second and pretest sessions ( P < 0.01), but it didn't significantly decreased and only approached to significant level between second and first test sessions ( P = 0.06). There was a significant difference between third with pretest ( P < 0.01) and third with first test sessions ( P = 0.03), but there was no significant difference between third and second test session's RT ( P = 1.0) for both groups [Table - 2], [Figure - 1]. Discussion Our results provide further evidence that bradykinesia can be improved by motor skill practice in PD patients in stage II. According to the results of this study, the group had a main effect on the RT, indicating that patients initiated the movements slower than healthy group and although RT decreased in patients as a result of hand-to-mouth practice, it was still lesser than healthy subjects. The significantly decreased RT at the first test session for both the groups, particularly in patients, demonstrated the immediate advantages of practice. Significantly decreased mean RT at the second test session as compared to the first test session in normal group, indicated that the benefits of one-week practice, but this was not significant and only approached significant level in patients which showed advantages of practice were reducing with extending of the practice period. More important to note was that the effects of practice on RT for both the groups were sustained after 1-week rest interval that no further practice was implemented, indicated that learning of motor skill practice influenced on information processing. The current finding that people with PD as well as normal persons being benefited and even more from one week motor skill practice is noticeable. The findings in the earlier studies had been different about the benefits of motor skill practice in PD patients. Some of these studies have presented a limited rate of performance improvement in people with PD as compared to normal subjects, as a result of motor learning impairments. [16],[21],[22] Other investigations [4],[12],[13] determined the positive effects of practice on performance and showed normal motor learning in PD patients. Studies by Agostino et al.[12] have demonstrated in patients with MD motor learning could be intact in spite of impairment of motor skills as a result of the disease. In the present study, two-day motor skill practice resulted in a parallel decrease in RT for both PD and control groups. With repetition of a motion, person's conscious effort is decreased and the motion becomes more and more automatic which is the goal of the rehabilitation. [23] The motor circuits of basal ganglia play a key role in the automatic execution of motor tasks. [24] Penhune and Doyon, [25] have demonstrated that cerebellar activity is high in the initiation of practice and with progressing of the practice from the first day to the fifth day, cerebellar activation decreases and basal ganglia activation increases. In our study, the gains of motor skill practice were reduced from second to seventh days and RT after seventh day of practice was not significant and just approached to significant level and this may reflect the impaired function of the basal ganglia in PD. Learning as a more permanent change of behavior, can only be inferred when improvement is maintained across time or transferred to different movement contexts. [6] Retention reflects how the kinematic improvement is maintained after ending of the practice. [3] In the present study, maintenance of the performance level after one-week retention period indicated a learning effect of motor skill practice. Movement variables responsible for retention may be encoded in a motor representation stored in distributed network of cortical motor area, including the primary motor, premotor, and parietal cortex. [25] Normal learning retention in people with PD may be demonstrated so that during execution of movements, some of the motor areas of cortex show hyperactivity, reflecting an attempt to compensate basal ganglia dysfunctions. [3] From a clinical and rehabilitation viewpoint, although we may not be able to generalize the results of our simple task to the complex daily performances, our finding that patients with mild to moderate PD can improve with motor skill practice, may be helpful in considering practice as a critical method and an effective rehabilitation intervention to decrease bradykinesia. [3],[4],[6] It should be mentioned that further follow-up studies on advantages at longer terms of motor skill practice and longer retention periods is warranted. Acknowledgments We wish to thank the staff of the Tajrish Hospital Parkinson's Clinic of Beheshti University of Medical Sciences for their valuable cooperation. I would also like to express my deepest appreciation to Dr. Parsa K, Dr. Pipelzadeh M, Taghizadeh G., and Keyhani M. for their invaluable comments and encouragements. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09214f1.jpg] [ni09214t2.jpg] [ni09214t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}