 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
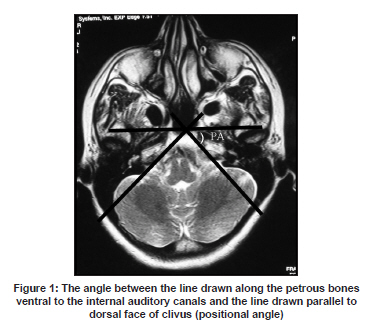
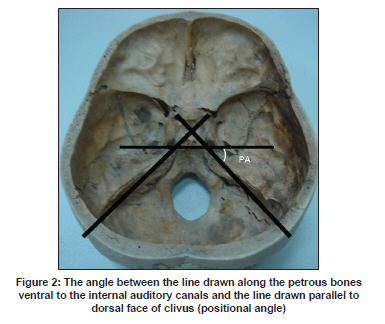
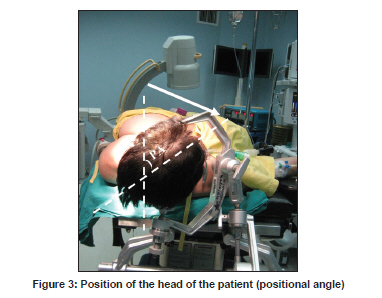
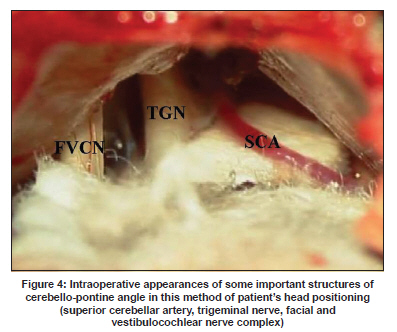
Neurology India, Vol. 57, No. 6, November-December, 2009, pp. 777-779 Technical Report A new method of patient's head positioning in suboccipital retrosigmoid approach Ersin Erdoğan, Erdinç Civelek, Mehmet Bülent Önal, İlker Solmaz, Cahit Kural, Hakan Yakupoğlu1 Department of Neurosurgery, Gülhane Military Medical Academy, 06100 Etlik, Date of Acceptance: 29-Sep-2009 Code Number: ni09216 PMID: 20139509 DOI: 10.4103/0028-3886.59476 Abstract Background: The retrosigmoid approach is a common route to the cerebellopontine angle and lateral clivus. Patient's head positioning just before the operation is crucial to perform the procedure effectively and safely.Aim : The aim of the study is to determine the positional angle of the head on preoperative axial sequences of the cranial magnetic resonance imaging (MRI). Materials and Methods : The angle between the line drawn along the petrous bone ventral to the internal auditory canal and the line drawn parallel to the dorsal face of the clivus on the axial view of MRI sequences was measured. Results : This method of patient positioning has resulted in minimal cerebellar retraction, less time in the preoperative preparation period and less postoperative headache and neck pain. Conclusions : This method can provide quick and better exposure of the cerebellopontine angle. Preoperative measurement of positional angle on axial MRI sequences is a very simple and sufficient way to determine the angle of the head that is turned to the contralateral side. Keywords: Cerebellopontine angle, retrosigmoid approach, head positioning, positional angle Introduction The retrosigmoid approach is a conventional approach for exploring the cerebellopontine angle lesions. This approach is considered the simplest route to the cerebellopontine angle and lateral clivus. This route may be used in a variety of surgeries, such as tumor removal, vestibular neurectomy, brainstem auditory implantation and neurovascular decompression. In this study, we aimed to assess the intraoperative positional angle of the head on preoperative magnetic resonance imaging (MRI). Angle measurement and the positioning The angle between the line drawn along the petrous bone ventral to the internal auditory canal and the line drawn parallel to the dorsal face of the clivus on printed films of an axial view of the MRI sequences was calculated using a goniometer and was named as the positional angle [Figure - 1] and [Figure - 2]. Patients were placed supine and the head was fixed by the Mayfield head clamp system. Using a goniometer, the head was turned to the other side of the surgical site as positional angle that was calculated before [Figure - 3]. Results The surgeon can sit at the surgical site of the patient's head with his or her feet under the table. An armrest for the surgeon may be placed for the arm nearest the vertex and the surgeon's other arm rests on the patient. During the operation, this method of patients' head positioning allows to identify important structures of the cerebellopontine angle [Figure - 4]. Advantages The important advantages of this procedure included: (1) Minimization of duration of the preoperative preparation, (2) less risk of postoperative head ache and neck pain resulting from extensive neck traction. Discussion The retrosigmoid approach is one of the commonly performed procedures of neurosurgical practice. It is the oldest approach to acoustic neuromas, first developed by Cushing and then refined by Dandy in the premicrosurgical era. [1] It is also used for microvascular decompression, [2] posterior inferior cerebellar artery aneurysms and access to the anterolateral brainstem as well as other cerebellopontine angle tumors. Many surgeons prefer the sitting/semisitting position for the retrosigmoid approach because it is more comfortable for the operator. [3],[4],[5] However, the important risk associated with the semisitting position is air embolism irrespective of close anesthetic monitoring. In addition, Samii et al. report a high incidence of hematoma formation after retrosigmoid removal of cystic tumors in the semisitting position. [3] In the semisitting position, the reduced intracranial venous pressure shrinks the peritumoral vein, which prevents troublesome intraoperative bleeding. In the lateral position, the peritumoral veins cause troublesome intraoperative bleeding and thus require hemostatis. [6] Supine position in retrosigmoid approach was discussed in the literature before. [1],[6] The method used by us avoids excessive head rotation and unnecessary ipsilateral shoulder elevation. Shoulder elevation using a pillow obscures the surgical field, especially in short-necked and overweighed patients. The most important advantages of this method are minimization of duration of the preoperative period and lessening of postoperative headache and neck pain resulting from extensive neck traction. This method is extremely useful, especially in patients with a significant limitation of neck motion. Minimum neck traction without injury to the occipital nerves can decrease incidence of postoperative headache and the patient's discomfort around the operation site. [7] The size of the petrous tubercle, depth of the posterior fossa, size of the cerebrospinal fluid spaces, venous anatomy and displacement of normal anatomy due to tumoral lesions may affect the surgery. During the operation, the line of sight to the brainstem and the petrous bone may be changed by rotating the operating table from side to side. There may not be the need for cerebellar retractors with proper patient positioning and adequate anesthesia techniques. After sufficient drainage of cerebrospinal fluid, with this method of patient positioning the need for cerebellar retraction will be minimal and there may not be any need for the use of cerebellar retractor system. This method can provide a quick and better exposure of the cerebellopontine angle. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09216f4.jpg] [ni09216f1.jpg] [ni09216f3.jpg] [ni09216f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}