 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
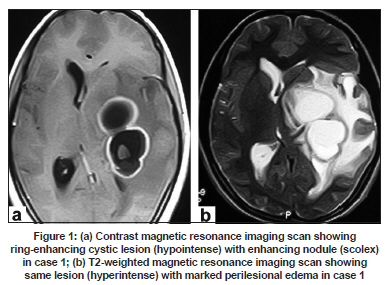
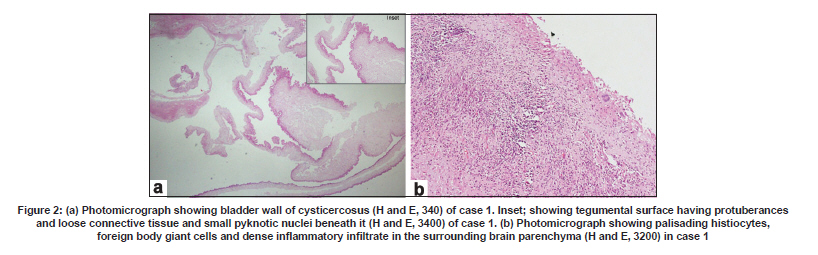
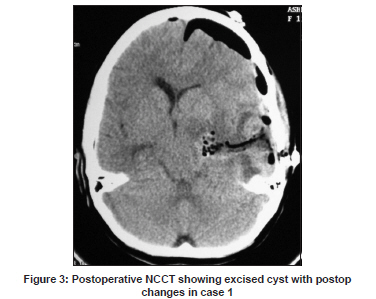
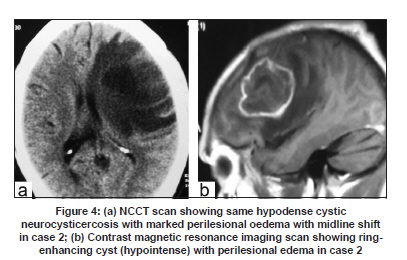
Neurology India, Vol. 57, No. 6, November-December, 2009, pp. 800-802 Case Report Giant intraparenchymal neurocysticercosis: Report of surgical aspects two cases Alok Umredkar, Navneet Singla, Sandeep Mohindra, Aman Bal 1 , Sunil Kumar Gupta Departments of Neurosurgery, and 1 Pathology, Postgraduate Institute of Medical Education and Research, Chandigarh, India Date of Acceptance: 09-Oct-2009 Code Number: ni09223 PMID: 20139516 DOI: 10.4103/0028-3886.59483 Abstract Giant parenchymal cysticercosis is a relatively rare condition and surgical treatment may be required when it is associated with elevated intracranial pressure. We report two patients with giant parenchymal cysticercosis who were treated surgically for the elevated intracranial pressure. In both the patients the preoperative diagnosis was of a cystic glioma. Total excision of the lesions was achieved in both the patients. In countries endemic to neurocysticercosis gaint parenchymal cysticercosis should be considered in the differential diagnosis of cystic enhancing mass lesion. Surgical excision may be indicated when it is associated with elevated intracranial pressure.Keywords: Cysticercosis, neurocysticercosis, taenia solium Introduction Neurocysticercosis (NCC) is the common parasitic infection worldwide. However, giant parenchymal cysticercosis, a lesion measuring more than 4 to 5 cm in its largest diameter and 60 mL in volume is uncommon. [1],[2] Giant cysts may not always be associated with elevated intracranial pressure, probably due to relatively slow growth of the lesion. [2] Elevated intracranial pressure is an ominous sign and may require surgery. [2] Diagnosis of NCC is often based on a combination of clinical features, radiological findings, serological and cerebrospinal (CSF) findings. [3] The treatment of NCC is mainly medical and surgery may be indicated in patients with mass effect and elevated intracranial pressure. We report two patients with gaint intraparenchymal cysticercosis who presented to the emergency department (ED) with elevated features of elevated intracranial pressure and were treated surgically with total excision of the lesion. Case Reports Case 1 A 17-year girl presented to the ED with 4 months history of headache, righted sided and altered mental status of one week duration. On examination, she was drowsy and had right-sided hemiparesis (motor power grade 4/5). Contrast magnetic resonance imaging (MRI) showed a large (5 x 4 x 3.5 cm) enhancing cystic lesion in the left insular and ganglionic region with an enhancing nodule compressing ipsilateral ventricle and perilesional edema [Figure - 1]a and b. The cyst was hypointense on T1-weighted image and hyperintense on T2-weighted image. The signal intensity of cyst was similar to CSF in all the sequences. With a preoperative diagnosis of either an abscess or a cystic glioma, she was taken up for surgery. A left temporoparietal craniotomy was done and a middle temporal gyrus approach was used. At operation the lesion was firm, fibrous, avascular and cystic with clear fluid. With microsurgical technique, the cystic lesion was dissected all around and excised. During dissection, the cyst ruptured. Histopathology showed brain parenchyma in multiple fragments, with extensive areas of central necrosis and cysticercosus parasite. The surrounding brain parenchyma showed a dense lymphoplasmacytic infiltrate, admixed with histiocytes and eosinophils, confirming the diagnosis of cysticercal cyst [Figure - 2]a and b. Postoperatively, she had worsening of motor power on the right side (grade 3/5) and transcortical motor aphasia which slowly recovered with speech therapy, physiotherapy. She was put on steroids and albendazole (15 mg/kg for 3 weeks). Postoperative CT scan showed total excision of the cyst [Figure - 3]. At 6 months follow-up, she had recovered almost completely. Case 2 A 40-year male presented to the ED with 2 months history of headache, seizure and altered mental status for last 1 week. On examination, he was drowsy and had right-sided hemiparesis (motor power grade 4/5). Non-contrast computerized tomography (CT) scan showed a large (5 x 4.5 x 4 cm) irregular hypodense cystic lesion in the left frontal region compressing ipsilateral ventricle and perilesional edema [Figure - 4]a. Contrast MRI demonstrated a ring enhancing cystic lesion and perilesional edema and significant mass effect [Figure - 4]b. As there was radiological evidence of herniation, he was taken up for surgery. The preoperative diagnostic considerations included glioma or infective lesion. At surgery, a firm, greyish, avascular cystic lesion with clear fluid was found. The lesion was excised totally. Histopathology confirmed the diagnosis of cysticercal cyst. Postoperatively, he had grade 3/5 hemiparesis. Patient was put on steroids and albendazole (15 mg/kg for 3 weeks) in the postoperative period. At 6 months follow-up, the patient had recovered fully and had no neurological deficits. Discussion Giant parenchymal cysticercosis is a relatively rare presentation of NCC and only few case reports have been published. [1],[2],[3],[4],[5],[6] Clinical presentation of NCC is quite variable and depends on: (i) location, growth, size and number of cysts; (ii) the stage of cyst - vesicular, degenerative, calcific; and (iii) host immune response. [4] Seizures are the most common presentation of NCC. Diagnosis of NCC is mostly based on the clinical, radiological, immunological and epidemiological parameters. [7] The diagnostic serological test of choice in NCC is electro-immuno transfer blot assay (EITB). It has near 100% specificity and 94-98% sensitivity in patients with two or more cysts. [8] MRI is the radiological investigation of choice to determine the pathological stage of cyst. [4] The stage of the cyst determines the MRI cyst morphology: Viable cysts show neither enhancement nor perilesional edema, and are hypointense to brain parenchyma. Contrast enhancement and perilesional edema are the MRI characteristics of cysts in the degenerative phase. The larval cyst is recognizable as a cystic structure but is obviously irreversibly damaged, and cystic fluid becomes more turbid, corresponding to the colloidal vesicular stage described by Escobar (1983). [1],[4] Based on the radiological features there appears two types giant intraparenchymal cysticercosis: (1) non- or mildly enhancing cystic type and (2) enhancing irregular type mimicking a glioblastoma multiforme. [7],[8],[9] In the first patient the lesion was cystic type and in the second patient the lesion resembled a malignant tumor. Large cystic lesions in NCC causing elevated intracranial pressure are more commonly seen in subarachnoid spacee. Because of the rarity the diagnosis of gaint intraparenchymal cysticercosis was not considered in both the patients. However, retrospective review of the films suggested the possibility of gaint intraparenchymal cysticercosis in the first patient. There was an enhancing nodule within the cyst, probably contrast enhancing scolex. However, in the second patient there were no such clues.for diagnosing gaint cysticercosis. The surgical approach for a large intraparenchymal cysticercosis should be by microsurgical dissection, carefully separating the thin-walled cyst from the surrounding brain parenchyma by peeling of arachnoid and saline irrigation. [9] No deleterious consequences secondary to intraoperative rupture were found in a study of 114 cases. [9] In the first patient although the cyst was opened at surgery, there was no parenchymal spread of the cyst fluid. This emphasizes the need to consider gaint intraparenchymal cysticercosis in the differential diagnosis of cystic enhancing lesions. This diagnosis should be considered in endemic countries particularly in patients presenting with a large cyst with CSF-like fluid and an enhancing wall with an eccentric nodule. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09223f2.jpg] [ni09223f4.jpg] [ni09223f3.jpg] [ni09223f1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}