 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
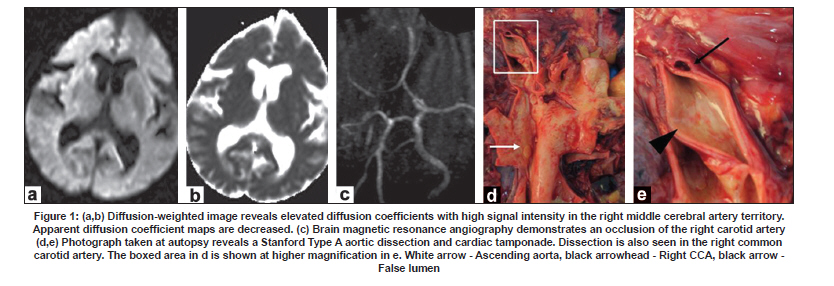
Neurology India, Vol. 57, No. 6, November-December, 2009, pp. 808-809 Letter To Editor Administration of recombinant tissue plasminogen activator to a case of cerebral infarction in the setting of painless aortic dissection Satoru Takeuchi, Yoshio Takasato, Hiroyuki Masaoka, Naoki Otani Department of Neurosurgery, National Hospital Organization Disaster Medical Center, Japan. Date of Acceptance: 12-May-2009 Code Number: ni09227 PMID: 20139520 DOI: 10.4103/0028-3886.59487 Sir, A 72-year-old female presented with acute onset left sided hemiparesis. On admission, a physical examination revealed a consciousness level of 15 on the Glasgow coma scale, blood pressure of 160/116 mmHg, and pulse rate of 51 per minute. Radial and femoral pulses were normal. Patient had left hmeparesis and National Institutes of Health Stroke Scale (NIHSS) score was 16. She did not complain any chest, abdominal and back pain. Chest X-ray, an electrocardiogram and brain computed tomography (CT) showed no abnormal findings. Brain magnetic resonance imaging (MRI) revealed a right middle cerebral artery territory infarct [Figure - 1]a and b. Brain MR angiography demonstrated an occlusion of right carotid artery [Figure - 1]c. Laboratory studies were within normal limits. One hundred and forty-four min after onset, the patient received recombinant tissue plasminogen activator (rt-PA), 39 mg (0.6 mg/kg). On Day 2, vital signs were stable and follow-up CT showed no hemorrhagic change. However, on Day 3, the patient suffered a sudden cardiac arrest from which she could not be resuscitated. Autopsy revealed a Stanford Type A aortic dissection (AD) and cardiac tamponade [Figure - 1]d. There was also dissection of the right common carotid artery [Figure - 1]d and e. Thrombolysis with rt-PA has been done in the setting of painless AD. [1] In our patient it is quite possible that the administration of rt-PA might have contributed to the death of the patient by the lysis of the thrombus that would otherwise have limited the dissection. Because AD is a rare cause of stroke, there is debate about the necessity to aggressively screen for AD. Although pain in the chest, back, or abdomen is a common symptom in AD, approximately 10% of patients experience no pain. [2],[3],[4],[5] Pulse and blood pressure differences and abnormal chest radiograms can be useful for the rapid assessment of AD. However, approximately 7% of AD patients show normal findings. [2] Color duplex ultrasound is a simple tool to exclude painless AD and cervical artery dissection. [3],[4] Chest CT scanning and transesophageal echocardiography, while very sensitive for AD, are time-consuming and expensive. [2],[3],[4] Strokes associated with AD are predominantly right hemispheric. [5] This dominance could be explained by varying mechanical dynamics in the progression of the dissecting hematoma. We believe a high index of suspicion of painless AD would be advisable and also a lower threshold for performing carotid ultrasound before rt-PA treatment, especially in patients with right hemispheric infarct. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09227f1.jpg] |
| |||||||||

{kind=link}