 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
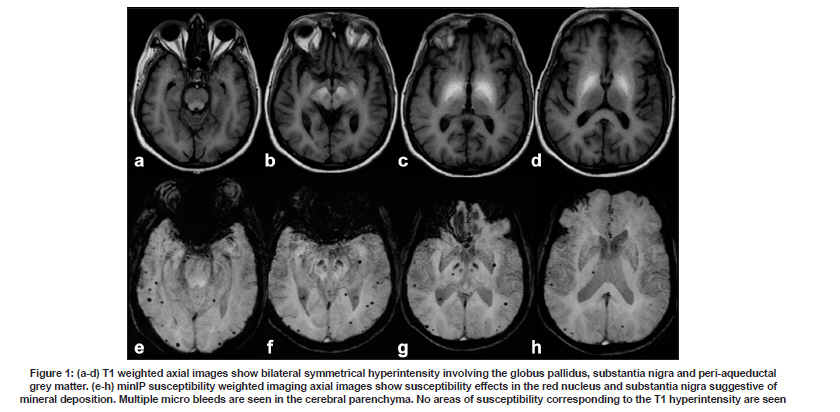
Neurology India, Vol. 57, No. 6, November-December, 2009, pp. 812-813 Letter To Editor Acquired hepatolenticular degeneration: Is the T1 hyperintensity due to manganese deposition? Neeraj N. Baheti, Haseeb Hassan, Chaturbhuj Rathore, Syam Krishnan, Chandrasekharan Kesavadas1 Departments of Neurology and 1 Imaging Sciences and Interventional Radiology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Thiruvananthapuram - 695 011, India. Date of Acceptance: 23-Oct-2009 Code Number: ni09229 PMID: 20139522 DOI: 10.4103/0028-3886.59489 Sir, Chronic liver failure associated extrapyramidal syndromes often occur without signs of hepatic encephalopathy and are associated with T1 hyperintensity in the pallidum on magnetic resonance (MR) imaging. This pallidal T1 hyperintensity has been attributed to manganese accumulation and elevated pallidal manganese concentrations are seen in cirrhotic patients dying from hepatic coma. [1],[2] Identical pallidal T1 hyperintensity is also seen in patients with neurotoxicity from welding fumes and experimental manganese loads in primates. [3] Susceptibility weighted imaging (SWI), a sensitive modality for detecting ferromagnetic and paramagnetic substances has never been used previously in imaging these patients. In this report, we describe our observations and discuss the plausible mechanism responsible for the findings. A 45-year-old man with chronic alcoholic liver disease was admitted to our institute with progressive symmetric rigid bradykinetic syndrome of three months duration with poor levodopa response. He had hypertension for the last five years and was on regular treatment. General physical examination revealed mild pallor and flapping tremors. Neurological examination showed mild frontal lobe dysfunction and symmetric rigidity, bradykinesia, gait ignition failure with marked freezing of gait and postural instability. He had no rest tremors or lateralizing signs. Systemic examination showed mild splenomegaly. Slit lamp examination for KF ring was negative. Plasma ammonia was 82 micromol/l and abdominal ultrasound showed evidence of chronic liver parenchymal disease, splenomegaly and minimal ascites. MR imaging showed bilateral symmetrical T1 hyperintensity involving the globus pallidus, substantia nigra and peri-aqueductal grey matter [Figure - 1] a-d. The SWI did not show increased susceptibility changes in the corresponding areas [Figure - 1] e-h. Incidental multiple micro bleeds were noted, most likely, related to hypertensive microangiopathy. The substantia nigra and red nucleus showed hypointensity due to age related mineral deposition. Manganese is a paramagnetic metal that shortens the T1 relaxation time sufficient to produce pallidal T1 hyperintensity in hepatolenticular degeneration. [4] Manganese is also used as MR contrast due to the above properties but surprisingly SWI failed to show any blooming. Interestingly, calcification containing diamagnetic calcium is visualized in SWI and hence is used in the seizure MR imaging protocol. [5] The magnetic susceptibility of paramagnetic manganese is much higher than diamagnetic calcium. [6] The association of manganese deposition and T1 hyperintensity is well known but the causation is not well established. In view of normal SWI many questions remain unanswered. Are there local tissue factors affecting the paramagnetic properties of accumulated manganese in basal ganglia? Is manganese accumulation just an inciting event and the observed T1 hyperintensity due to some other cause? In cases with hepatolenticular degeneration, microscopic examination of the pallidum shows Alzheimer type II astrocytes without any calcification, melanin deposition or hemorrhage to account for the T1 hyperintensity. [1] Primate and human studies have shown that astrocytic accumulation of manganese increases glutamate/glutamine with simultaneous decrease in myo-inositol, inducing selective neuronal loss in the basal ganglia structures and reactive gliosis (Alzheimer type II astrocytes). [2],[3] The T1 hyperintensity may be due to the intracellular macromolecule accumulation due to energy failure or could result from the protein hydration layer inside the cytoplasm of astrocytes. [2],[7] Further studies delving into these issues are needed to understand the pathological mechanisms underlying T1 hyperintensity in acquired hepatolenticular degeneration. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09229f1.jpg] |
| |||||||||

{kind=link}