 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
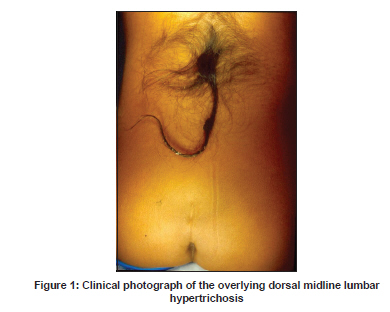
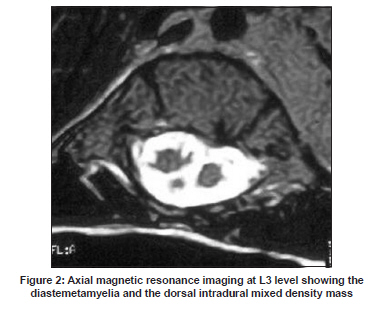
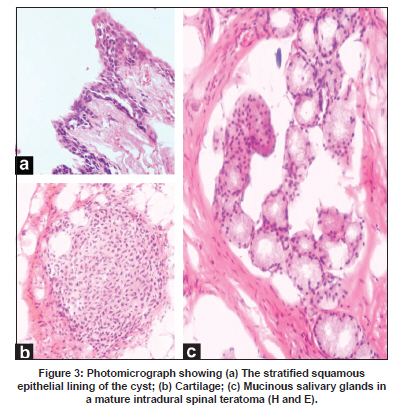
Neurology India, Vol. 57, No. 6, November-December, 2009, pp. 821-822 Letter To Editor Spinal teratoma with salivary glandular differentiation A. M. Shubha, Suravi Mohanty1 , Kanishka Das, Isha Garg1 Departments of Paediatric Surgery and 1 Pathology, St. John’s Medical College Hospital, St. John’s National Academy of Health Sciences, Bangalore - 560 034, India Date of Acceptance: 22-Feb-2009 Code Number: ni09234 PMID: 20139527 DOI: 10.4103/0028-3886.59494 Sir, Spinal dysraphism encompasses a spectrum of congenital spinal anomalies resulting from failure of dysjunction of the surface ectoderm forming the skin and dermal appendages from the neuroectoderm forming the spinal cord between the third and eighth week of gestation. [1] Congenital inclusion tumors (CIT) refer to lesions arising from disordered embryogenesis and entrapment of different germ layers within the developing spinal cord and include epidermoids, dermoids, and teratomas. Intraspinal dermoids account for 17% of primary spinal tumors during infancy and for 13% in children below 15 years of age. [2] The occurrence of intradural spinal teratomas with spinal dysraphism is even more uncommon. [3] We describes an intradural spinal teratoma containing mucous salivary glands in a patient with occult spinal dysraphism and diastemetamyelia. A 12-year-old, presented with an occasional diurnal and nocturnal urinary dribble and soiling of the undergarments since three months. Her voiding and bowel habits were otherwise normal and she had no motor deficits. Besides a midline hypertrichosis at the L1-5 level [Figure - 1], the neurological examination was normal. Plain X-ray showed a spina bifida at L3-4, while the T1-weighted magnetic resonance imaging (MRI) demonstrated a low lying conus (L4), a wide lumbar thecal sac (L1-5), and the cord tethered by a ventral bony diastemetamyelia (L3). Additionally, there was a heterogenous mixed intensity dorsal intradural mass at L3 [Figure - 2]. The renal function tests and urinary tract ultrasonography were normal. A three vertebrae (L2-4) laminectomy, microsurgical excision of the bony diastem, and the intraspinal mass was done. The operative findings matched the preoperative MRI details. The dorsal intradural cystic solid mass was moderately adherent to the surrounding tissues and contained a mix of firm cartilaginous structure and thick mucoid material. Microscopically, it showed tridermal differentiation of a mature teratoma with foci of stratified squamous epithelium, immature cartilage, and mucous salivary glands [Figure - 3]. The patient made an uneventful recovery; the indwelling bladder catheter was removed after a week and the urinary dribble had completely resolved at the first follow-up visit at three weeks after the surgery. At four years follow up, she is asymptomatic and well. Failure of an orderly separation of the neuroectoderm from the surface ectoderm with the interposition of mesoderm (dysjunction) results in a spectrum of defects involving the skin, spinal cord, as well as the intervening mesodermal structures. Errors in dysjunction manifest as a variety of spinal dysraphic states including dermal sinus tracts (DSTs) and CITs. [4] Spinal dysraphism is seen in 2-4/1000 live births. Spinal DSTs have an incidence of 1 in 2500 live births and are common in the lumbosacral region. [5] CITs such as epidermoids, dermoids, and teratomas form along the DSTs till the spinal cord or within it. In occult spinal dysraphism, the most frequent reason for referral is a cutaneous finding; however, many already have neurologic deficits at presentation. About 50% of a large series of DSTs had an associated intradural mass lesion. [4] CITs exist at birth are overtly symptomatic in infancy, adolescence, or adulthood because of a characteristic slow growth. [6] DSTs and associated CITs may lead to spinal cord tethering and progressive neurological deterioration. In this case, despite the obvious overlying hypertrichosis, physician attention was sought only after the onset of the urinary dribble. The presence of an intradural teratoma in association with spinal dysraphism is extremely rare. Anecdotal reports have described tertomas with split cord malformations, myelomeningocele, and lipomyelomeningocele. [3],[7] Despite a relatively delayed adolescent presentation, our patient had a relatively short duration of urinary incontinence and made a complete neurologic recovery postoperatively. Though some researchers have suggested a neoplastic transformation of heterotopic primordial elements during neural tube embryogenesis, [8] most believe that these tumors are more dysembryogenetic than neoplastic. [3] Teratomas contain derivatives from all three embryonic layers (tridermal); they are termed mature or immature depending on the differentiation of elements. Besides the usual admixture of skin and adnexal elements, muscle, fat, neural tissue, bone, and cartilage, mature intradural spinal teratomas with intestinal, respiratory, and renal tissue have also been reported. [3],[9] This intradural spinal teratoma with a lumbar split cord malformation showed a mature tridermal differentiation and the endodermal component was represented by mucous salivary glands. This is probably the first report of salivary glandular differentiation in a spinal teratoma. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09234f2.jpg] [ni09234f1.jpg] [ni09234f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}