 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
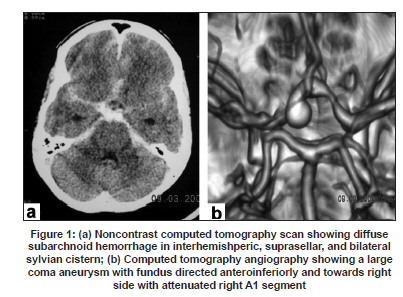
Neurology India, Vol. 57, No. 6, November-December, 2009, pp. 826-828 Letter To Editor Ruptured anterior communicating artery aneurysm presenting with monocular blindness Alok A. Umredkar, Navneet Singla, Sunil K. Gupta Department of Neurosurgery, Postgraduate Institute of Medical Education and Research, Chandigarh, India. Date of Acceptance: 02-Jul-2009 Code Number: ni09238 PMID: 20139531 DOI: 10.4103/0028-3886.59498 Sir, Subarchnoid hemorrhage (SAH) is the common presenting feature of anterior communicating artery (Acoma) aneurysms. The usual locations of the aneurysms presenting with visual deficits are cavernous, carotid-ophthalmic, supraclinoid, paraclinoid, posterior communicating. [1] Only a few cases of Acoma aneurysms presenting with visual deficits have been reported in the literature. [1],[2],[3] A 45-year-old female patient presented in emergency with sudden onset headache, vomiting, and right eye vision loss. Vision loss was sudden and complete. On examination, she was conscious and well oriented. Her vision and pupil on left side was normal, whereas on right side there was no perception of light; right pupil was dilated and nonreacting. She also had neck stiffness. Cranial computed tomography (CT) scan showed diffuse SAH in anterior interhemispheric fissure, suprasellar cistern, and bilateral sylvian fissures [Figure - 1]a. CT angiography showed a large pedunculated Acoma aneurysm 75 x 45 x 35 mm 3 with fundus directed anteroinferiorly, towards right side with 3 mm long and narrow neck (2 mm); and right A1 segment was attenuated [Figure - 1]b. She was subjected to pterional craniotomy and clipping of Acoma aneurysm. Intraoperatively, the Acoma aneurysm was found to be projecting into right optic nerve. There was dense adhesion between the aneurysm sac and the optic nerve with evidence of hemorrhage into the nerve. Gently aneurysm was dissected and was clipped with an asculap permanent 6.5 mm curved clip. There was no intraoperative rupture and no temporary clipping was used. Postoperative period was uneventful. Vision in the right eye did not improve. At one year follow-up, patient was fully conscious and oriented, but the vision in the right eye had still not improved. Ruptured Acoma aneurysms generally present with SAH and associated focal neurological deficits. The various causes of visual deficits include: Compression of the optic apparatus, [1] leaking of aneurysm inside the optic nerve or chiasma, [2] perianeurysmal inflammatory changes, [3] thromboembolism, and vitreous hemorrhage (terson's syndrome). [4] Only a few ruptured Acoma aneurysms with visual deficits such as monocular blindness have been reported till date. [1],[2],[3] In most of the patients visual deficits were related to chiasmal field defects because of the proximity of Acoma complex to the optic chiasma rather than optic nerve. Isolated involvement of one optic nerve resulting in monocular blindness has not been reported before. In the present case, monocular blindness was probably due to the direction of the growth of fundus of large Acoma aneurysm and compression of the optic nerve and also due to the hemorrhage into the optic nerve., Distortion or traction and indirect pressure on the optic nerves at the margins of the optic foramina also play an important role. [3] Other factor is interference with the blood supply of the optic nerve or chiasma either by occlusion or distortion of the perforating arteries arising from anterior cerebral-communicating complex. In large Acoma aneurysms, the intraaneurysmal thrombosis may occlude the origins of the branch vessels supplying the optic nerves and chiasma and thus causing ischemia. Sometimes, if the optic nerve is adherent to the fundus of the Acoma aneurysm there may also be damage from hemorrhage into the neural substance. [3] This was the most likely cause of monocular blindness in our case. This was also confirmed intraoperatively as fundus of Acoma aneurysm was compressing the optic nerve with hemorrhagic staining of the optic nerve. Patients with unruptured aneurysms may present only with progressive visual loss, due to the compression of optic pathway by enlarging aneurysmal sac or other causes. Thus neurologists, neurosurgeons, and ophthalmologists should have high index of suspicion and should consider unruptured Acoma aneurysm as one of the differential diagnosis for monocular blindness. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09238f1.jpg] |
| |||||||||

{kind=link}