 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
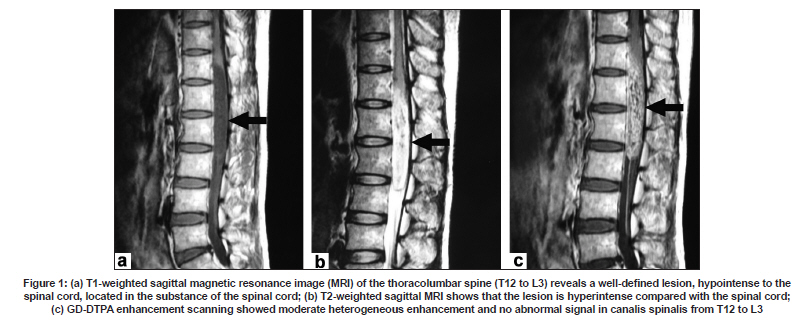
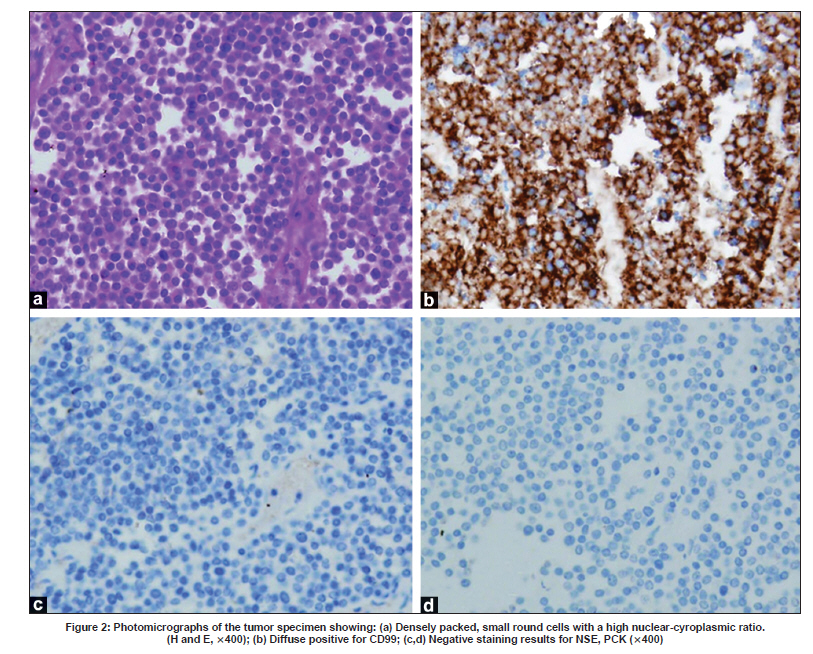
Neurology India, Vol. 57, No. 6, November-December, 2009, pp. 828-829 Letter To Editor Intramedullary Ewing's sarcoma of the spinal cord associated with hydrocephalus Lu Jia, Guoping Li, Chao You, Min He, Feng Ye Department of Neurosurgery, West China Hospital of Sichuan University, 37 Guo Xue Xiang, Wu Hou District, Chengdu - 610 041, China. Date of Acceptance: 02-Jul-2009 Code Number: ni09239 PMID: 20139532 DOI: 10.4103/0028-3886.59499 Sir, Ewing's sarcoma is an uncommon malignant tumor and accounts for approximately 10% of the primary malignant bone tumors. [1] Spinal cord metastases is an extremely rare and only two cases have been reported. [2],[3] We report a third patient. A 28-year-old man presented with progressive weakness of both lower extremities of fifteen days duration and recurrent headaches, vomiting, fever and bladder of four days duration and bowel incontinence of one day duration.Neurological examination showed bilateral papilledema and abducens nerve paralysis. Flaccid areflexic weakness (motor power 0/5) in both the lower with sensory level at T11 for all the modalities of sensations. Cranial magnetic resonance imaging (MRI) showed communicating type of hydrocephalus. Spintal MRI showed abnormal signal focus (14 x 2 x 2 cm 3 ) at the level of T12 to L3 vertebrae [Figure - 1]a-c. External ventricular drainage and exploration and decompression of spinal canal from T11 to L3 were performed. During the operation, spinal exploration found sclerotin of vertebra bodies from T11 to L3 as normal. The tumor was flesh and soft, with no clear boundary and peplos. The gross tumor was resected under micromanipulation. Both hematoxylin and eosin (H and E) and immunohistochemistry staining [Figure - 2] made the diagnosis of Ewing's sarcoma. The patient recovered well. But the sarcoma recurred and metastasis nine months after the operation, and there was no more opportunity to treat the disease. Ewing's sarcoma is a kind of osseous undifferentiated reticulocytic sarcoma, which was firstly reported in 1921 by James Ewing. It represents the second most common primary bone malignancy in childhood and adolescence, with an estimated annual incidence of 0.6 per million population. [4] It was depicted that the Ewing's sarcoma was originated from immature marrow reticulum tissue, while more and more immunohistochemistry, electron microscope and cytogene studies on sarcoma indicate the tumor originated from neural ectoderm. [2],[5] In this report, the tumor was originated from nerve tissue in the spinal cord. Neither clinical and MRI examination nor the operation indicated any relationship between tumor and sclerotin, and the spondylous was intact. Initial symptoms of intramedullary Ewing's sarcoma were completely similar to common tumor in the spinal cord, which included decreasing sensation or absence first and followed by motor dysfunction and difficulty of urination and defecation. However, intramedullary Ewing's sarcoma had an acute onset and a short course of disease, and a progressive aggravation of nerve damage, which caused the complete flaccid paralysis. Being short of vigilance and perceptual ability were the main reasons for the early misdiagnosis. The patient was wrongly diagnosed as cerebral meningitis because of the ardent fever and headache after the disease appeared. Three times failure of lumbar puncture as well as the cerebral meningitis irritation symptoms made therapy of infectious disease to be conducted. Only when both lower extremities paralysis and urinary and fecal incontinence happened after the fourth lumbar puncture, intramedullary Ewing's sarcoma was detected by the spinal cord MRI inspection. Therefore, whenever came to diseases in the spinal cord that were acute and together with fever or dropsy of brain with acute intracranial hypertension, intramedullary Ewing's sarcoma should be considered first. Overall, low T1WI signal and high T2WI signal spinal cord MRI together with moderate enhancement effect in a young adult with fever was considered as intramedullary Ewing's sarcoma. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09239f2.jpg] [ni09239f1.jpg] |
| |||||||||

{kind=link}
{kind=link}